Department of Medicine, University of California, San Francisco, CA.
Department of Medicine, San Francisco Veterans Affairs Medical Center, University of California, San Francisco, CA.
J Am Heart Assoc. 2016 Dec 20;5(12):e004243. doi: 10.1161/JAHA.116.004243.
Compared to uninfected adults, HIV-infected adults on antiretroviral therapy are at increased risk of cardiovascular disease. Given the increase in T-cell dysfunction, inflammation, and coagulation in HIV infection, microvascular dysfunction is thought to contribute to this excess cardiovascular risk. However, the relationships between these variables remain undefined.
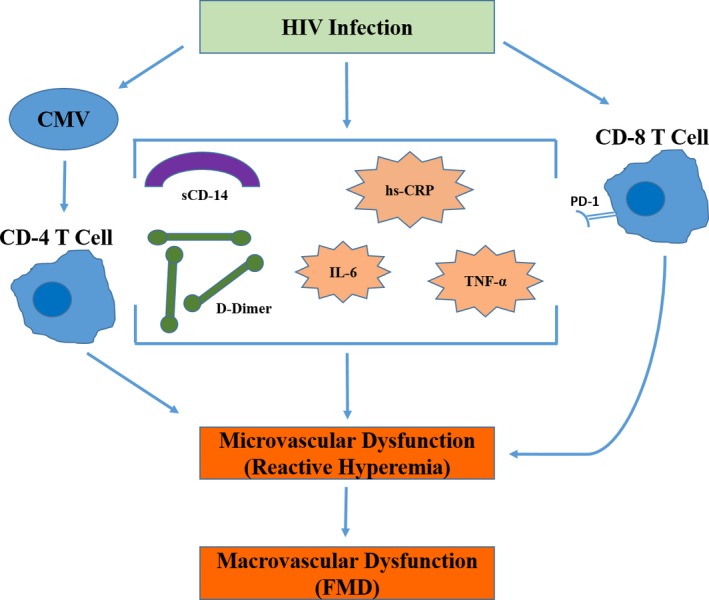
This was a cross-sectional study of 358 HIV-infected adults from the SCOPE cohort. Macrovascular endothelial function was assessed using flow-mediated dilation of the brachial artery and microvascular function by reactive hyperemia. T-cell phenotype was determined by flow cytometry. Plasma markers of inflammation (tumor necrosis factor-α, interleukin-6, high-sensitivity C-reactive protein, sCD14) and coagulation (fibrinogen, D-dimer) were also measured. In all HIV+ subjects, markers of inflammation (tumor necrosis factor-α, high-sensitivity C-reactive protein), coagulation (D-dimer) and T-cell activation (CD8+PD1+, CD4+interferon+cytomegalovirus-specific) were associated with worse reactive hyperemia after adjusting for traditional cardiovascular risk factors and co-infections. In treated and suppressed subjects, tumor necrosis factor-α and CD8+PD1+ cells remained associated with worse reactive hyperemia after adjustment. Compared to the untreated subjects, CD8+PD1+ cells were increased in the virally suppressed group. Reactive hyperemia was predictive of flow-mediated dilation.
CD8+PD1+ cells and tumor necrosis factor-α were associated with microvascular dysfunction in all HIV+ subjects and the treated and suppressed group. Additionally, D-dimer, high-sensitivity C-reactive protein, sCD-14, and interleukin-6 were associated with microvascular dysfunction in all HIV+ subjects. Although T-cell dysfunction, inflammation, and microvascular dysfunction are thought to play a role in cardiovascular disease in HIV, this study is the first to look at which T-cell and inflammatory markers are associated with microvascular dysfunction in HIV-infected individuals.
与未感染的成年人相比,接受抗逆转录病毒治疗的 HIV 感染者发生心血管疾病的风险增加。鉴于 HIV 感染中 T 细胞功能障碍、炎症和凝血的增加,微血管功能障碍被认为是导致这种心血管风险增加的原因。然而,这些变量之间的关系尚未明确。
这是一项来自 SCOPE 队列的 358 名 HIV 感染者的横断面研究。通过肱动脉血流介导的扩张来评估大血管内皮功能,通过反应性充血来评估微血管功能。通过流式细胞术确定 T 细胞表型。还测量了炎症(肿瘤坏死因子-α、白细胞介素-6、高敏 C 反应蛋白、sCD14)和凝血(纤维蛋白原、D-二聚体)的血浆标志物。在所有 HIV+受试者中,炎症标志物(肿瘤坏死因子-α、高敏 C 反应蛋白)、凝血标志物(D-二聚体)和 T 细胞激活标志物(CD8+PD1+、CD4+干扰素+巨细胞病毒特异性)与调整传统心血管危险因素和合并感染后反应性充血较差相关。在接受治疗和抑制病毒的受试者中,调整后肿瘤坏死因子-α和 CD8+PD1+细胞仍与反应性充血较差相关。与未治疗的受试者相比,病毒抑制组的 CD8+PD1+细胞增加。反应性充血可预测血流介导的扩张。
CD8+PD1+细胞和肿瘤坏死因子-α与所有 HIV+受试者以及治疗和抑制病毒的组的微血管功能障碍相关。此外,D-二聚体、高敏 C 反应蛋白、sCD-14 和白细胞介素-6与所有 HIV+受试者的微血管功能障碍相关。尽管 T 细胞功能障碍、炎症和微血管功能障碍被认为在 HIV 中的心血管疾病中起作用,但这项研究首次观察了哪些 T 细胞和炎症标志物与 HIV 感染者的微血管功能障碍相关。