Sluyter J D, Hughes A D, Thom S A McG, Lowe A, Camargo C A, Hametner B, Wassertheurer S, Parker K H, Scragg R K R
School of Population Health, University of Auckland, Auckland, New Zealand.
Institute of Cardiovascular Sciences, University College London, London, UK.
J Hum Hypertens. 2017 May;31(5):305-312. doi: 10.1038/jhh.2016.78. Epub 2016 Dec 22.
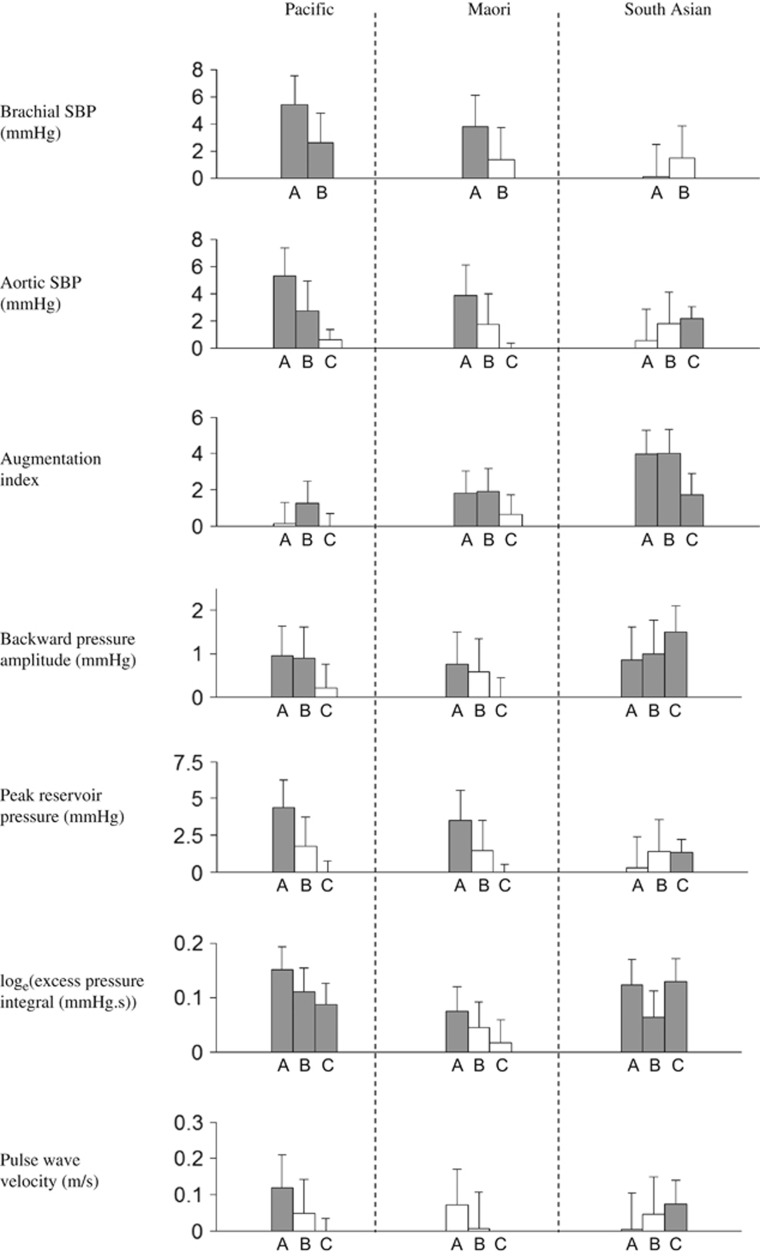
Little is known about how aortic waveform parameters vary with ethnicity and lifestyle factors. We investigated these issues in a large, population-based sample. We carried out a cross-sectional analysis of 4798 men and women, aged 50-84 years from Auckland, New Zealand. Participants were 3961 European, 321 Pacific, 266 Maori and 250 South Asian people. We assessed modifiable lifestyle factors via questionnaires, and measured body mass index (BMI) and brachial blood pressure (BP). Suprasystolic oscillometry was used to derive aortic pressure, from which several haemodynamic parameters were calculated. Heavy alcohol consumption and BMI were positively related to most waveform parameters. Current smokers had higher levels of aortic augmentation index than non-smokers (difference=3.7%, P<0.0001). Aortic waveform parameters, controlling for demographics, antihypertensives, diabetes and cardiovascular disease (CVD), were higher in non-Europeans than in Europeans. Further adjustment for brachial BP or lifestyle factors (particularly BMI) reduced many differences but several remained. Despite even further adjustment for mean arterial pressure, pulse rate, height and total:high-density lipoprotein cholesterol, compared with Europeans, South Asians had higher levels of all measured aortic waveform parameters (for example, for backward pressure amplitude: β=1.5 mm Hg; P<0.0001), whereas Pacific people had 9% higher log (excess pressure integral) (P<0.0001). In conclusion, aortic waveform parameters varied with ethnicity in line with the greater prevalence of CVD among non-white populations. Generally, this was true even after accounting for brachial BP, suggesting that waveform parameters may have increased usefulness in capturing ethnic variations in cardiovascular risk. Heavy alcohol consumption, smoking and especially BMI may partially contribute to elevated levels of these parameters.
关于主动脉波形参数如何随种族和生活方式因素而变化,我们所知甚少。我们在一个基于人群的大样本中对这些问题进行了调查。我们对来自新西兰奥克兰的4798名年龄在50 - 84岁的男性和女性进行了横断面分析。参与者包括3961名欧洲人、321名太平洋岛民、266名毛利人和250名南亚人。我们通过问卷评估了可改变的生活方式因素,并测量了体重指数(BMI)和肱动脉血压(BP)。采用超收缩振荡法得出主动脉压力,并据此计算出多个血流动力学参数。大量饮酒和BMI与大多数波形参数呈正相关。当前吸烟者的主动脉增强指数水平高于非吸烟者(差异 = 3.7%,P < 0.0001)。在控制了人口统计学因素、抗高血压药物、糖尿病和心血管疾病(CVD)后,非欧洲人的主动脉波形参数高于欧洲人。进一步调整肱动脉血压或生活方式因素(尤其是BMI)减少了许多差异,但仍有一些差异存在。尽管进一步调整了平均动脉压、脉率、身高以及总高密度脂蛋白胆固醇,但与欧洲人相比,南亚人所有测量的主动脉波形参数水平更高(例如,对于反向压力幅度:β = 1.5 mmHg;P < 0.0001),而太平洋岛民的对数(超压积分)高9%(P < 0.0001)。总之,主动脉波形参数随种族而变化,这与非白人人群中CVD患病率较高一致。一般来说,即使在考虑了肱动脉血压之后也是如此,这表明波形参数在捕捉心血管风险的种族差异方面可能具有更大的用途。大量饮酒、吸烟,尤其是BMI可能部分导致这些参数水平升高。