Neumann Peter J, Thorat Teja, Zhong Yue, Anderson Jordan, Farquhar Megan, Salem Mark, Sandberg Eileen, Saret Cayla J, Wilkinson Colby, Cohen Joshua T
Center for the Evaluation of Value and Risk in Health, Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, United States of America.
PLoS One. 2016 Dec 22;11(12):e0168512. doi: 10.1371/journal.pone.0168512. eCollection 2016.
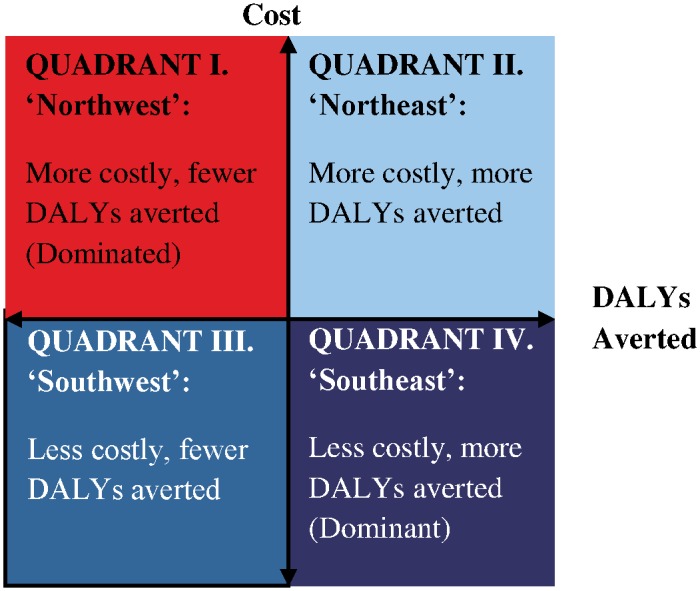
Calculating the cost per disability-adjusted life years (DALYs) averted associated with interventions is an increasing popular means of assessing the cost-effectiveness of strategies to improve population health. However, there has been no systematic attempt to characterize the literature and its evolution.
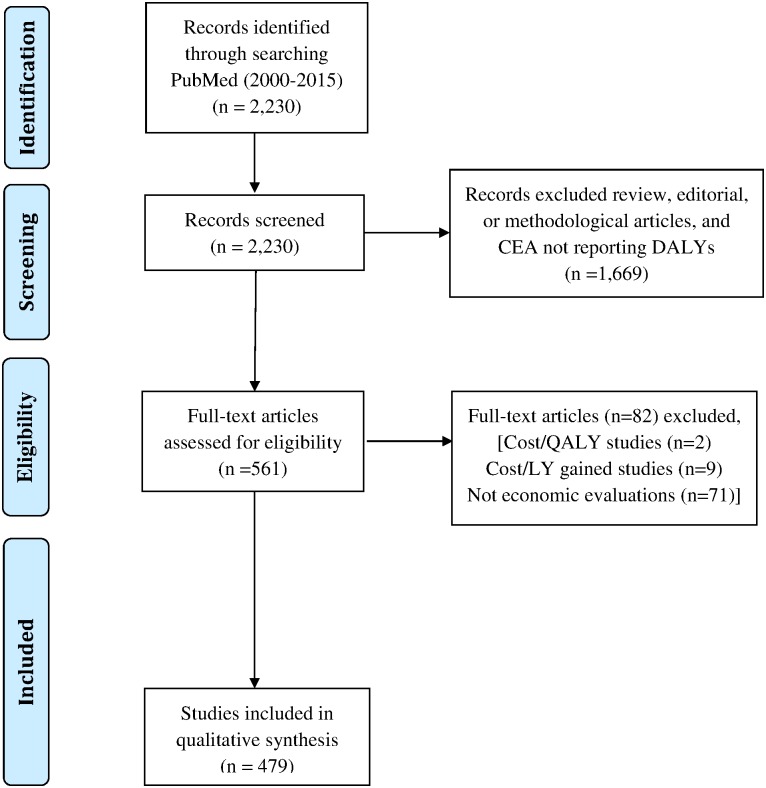
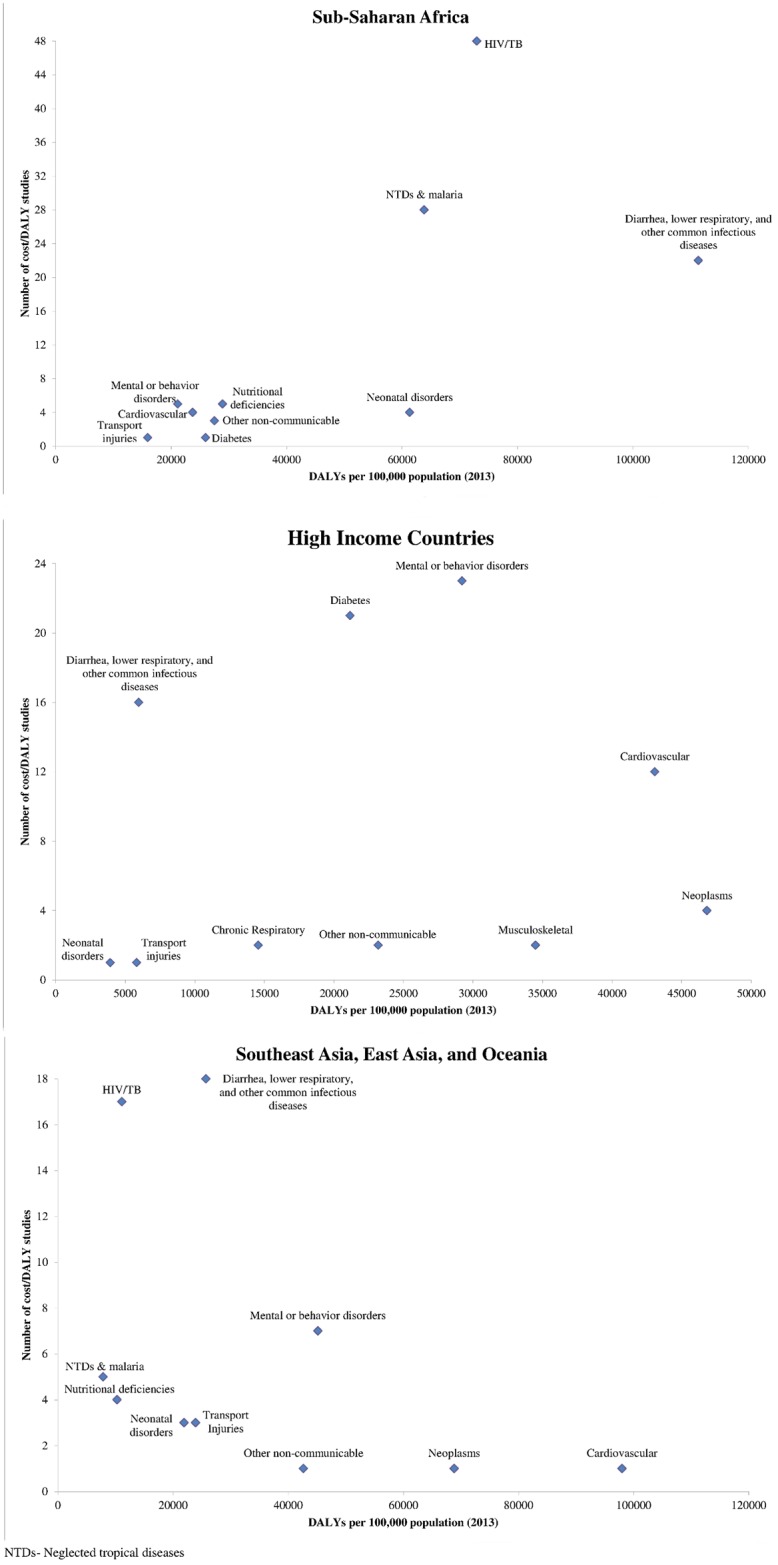
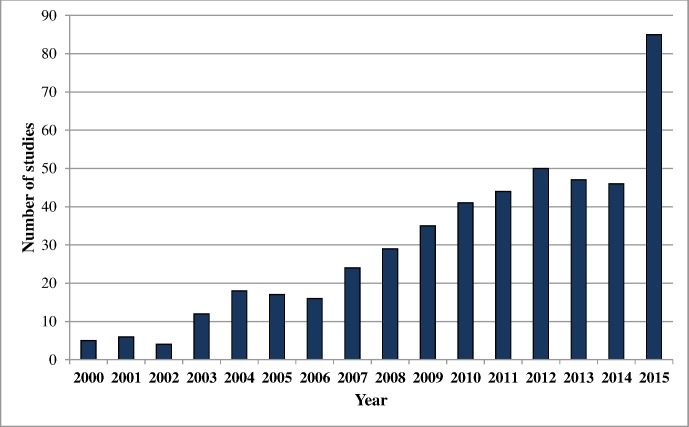
We conducted a systematic review of cost-effectiveness studies reporting cost-per-DALY averted from 2000 through 2015. We developed the Global Health Cost-Effectiveness Analysis (GHCEA) Registry, a repository of English-language cost-per-DALY averted studies indexed in PubMed. To identify candidate studies, we searched PubMed for articles with titles or abstracts containing the phrases "disability-adjusted" or "DALY". Two reviewers with training in health economics independently reviewed each article selected in our abstract review, gathering information using a standardized data collection form. We summarized descriptive characteristics on study methodology: e.g., intervention type, country of study, study funder, study perspective, along with methodological and reporting practices over two time periods: 2000-2009 and 2010-2015. We analyzed the types of costs included in analyses, the study quality on a scale from 1 (low) to 7 (high), and examined the correlation between diseases researched and the burden of disease in different world regions.
We identified 479 cost-per-DALY averted studies published from 2000 through 2015. Studies from Sub-Saharan Africa comprised the largest portion of published studies. The disease areas most commonly studied were communicable, maternal, neonatal, and nutritional disorders (67%), followed by non-communicable diseases (28%). A high proportion of studies evaluated primary prevention strategies (59%). Pharmaceutical interventions were commonly assessed (32%) followed by immunizations (28%). Adherence to good practices for conducting and reporting cost-effectiveness analysis varied considerably. Studies mainly included formal healthcare sector costs. A large number of the studies in Sub-Saharan Africa addressed high-burden conditions such as HIV/AIDS, tuberculosis, neglected tropical diseases and malaria, and diarrhea, lower respiratory infections, meningitis, and other common infectious diseases.
The Global Health Cost-Effectiveness Analysis Registry reveals a growing and diverse field of cost-per-DALY averted studies. However, study methods and reporting practices have varied substantially.
计算与干预措施相关的每避免一个伤残调整生命年(DALY)的成本,是评估改善人群健康策略成本效益的一种越来越流行的方法。然而,尚未有系统的尝试来描述该文献及其演变情况。
我们对2000年至2015年期间报告每避免一个DALY成本的成本效益研究进行了系统综述。我们建立了全球卫生成本效益分析(GHCEA)登记库,这是一个在PubMed中索引的英文每避免一个DALY成本研究的储存库。为了识别候选研究,我们在PubMed中搜索标题或摘要中包含“伤残调整”或“DALY”短语的文章。两名接受过卫生经济学培训的评审员独立评审我们摘要评审中选出的每篇文章,使用标准化数据收集表收集信息。我们总结了研究方法的描述性特征:例如,干预类型、研究国家、研究资助者、研究视角,以及两个时间段(2000 - 2009年和2010 - 2015年)的方法和报告实践。我们分析了分析中包含的成本类型、研究质量(从1(低)到7(高)评分),并研究了所研究疾病与不同世界区域疾病负担之间的相关性。
我们确定了2000年至2015年期间发表的479项每避免一个DALY成本的研究。撒哈拉以南非洲的研究占已发表研究的最大部分。最常研究的疾病领域是传染病、孕产妇、新生儿和营养障碍(67%),其次是非传染性疾病(28%)。很大一部分研究评估了一级预防策略(59%)。药物干预措施经常被评估(32%),其次是免疫接种(28%)。在进行和报告成本效益分析时对良好实践的遵循情况差异很大。研究主要包括正规医疗部门的成本。撒哈拉以南非洲的大量研究涉及高负担疾病,如艾滋病毒/艾滋病、结核病、被忽视的热带病和疟疾,以及腹泻、下呼吸道感染、脑膜炎和其他常见传染病。
全球卫生成本效益分析登记库揭示了一个不断发展且多样化的每避免一个DALY成本研究领域。然而,研究方法和报告实践差异很大。