Nishino Mizuki, Ramaiya Nikhil H, Chambers Emily S, Adeni Anika E, Hatabu Hiroto, Jänne Pasi A, Hodi F Stephen, Awad Mark M
Department of Radiology, Brigham and Women's Hospital and Dana-Farber Cancer Institute, 450 Brookline Ave., Boston, MA 02215 USA.
Department of Medical Oncology and Department of Medicine Dana-Farber Cancer Institute and Brigham and Women's Hospital, 450 Brookline Ave., Boston, MA 02215 USA.
J Immunother Cancer. 2016 Dec 20;4:84. doi: 10.1186/s40425-016-0193-2. eCollection 2016.
Tumor response characteristics using immune-related RECIST1.1 (irRECIST1.1) in advanced non-small-cell lung cancer (NSCLC) patients treated with nivolumab monotherapy in the clinical setting have not been previously described with a direct comparison with the assessments according to the conventional RECIST1.1.
Fifty-six advanced NSCLC patients treated with nivolumab monotherapy after its Food and Drug Administration (FDA) approval were retrospectively studied. Tumor burden was quantified on serial CT scans during therapy using irRECIST1.1, which uses unidimensional measurements and includes new lesion measurements in total tumor burden. Response assessments by irRECIST1.1 were compared with assessments by RECIST1.1. Responses of individual lesions in different organs were also compared.
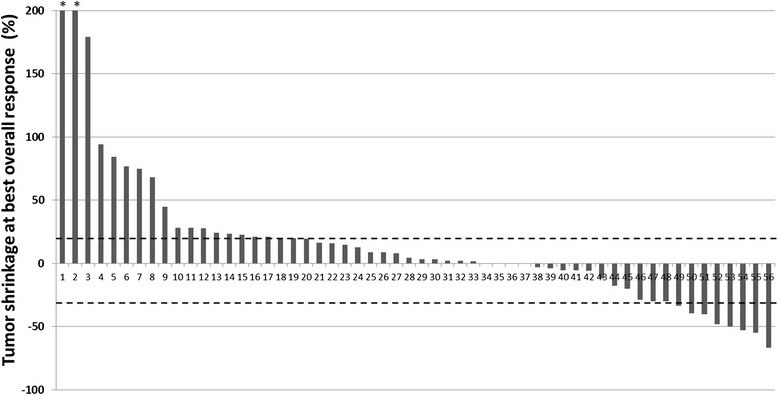
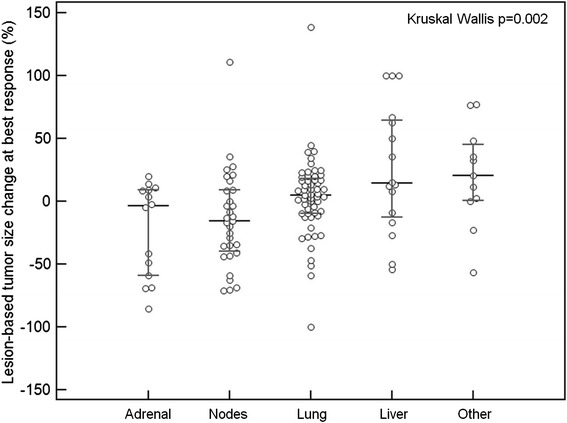
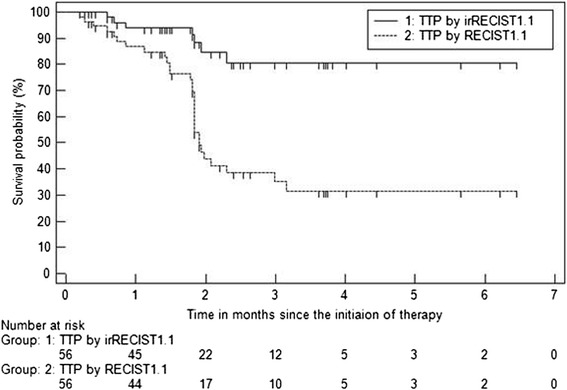
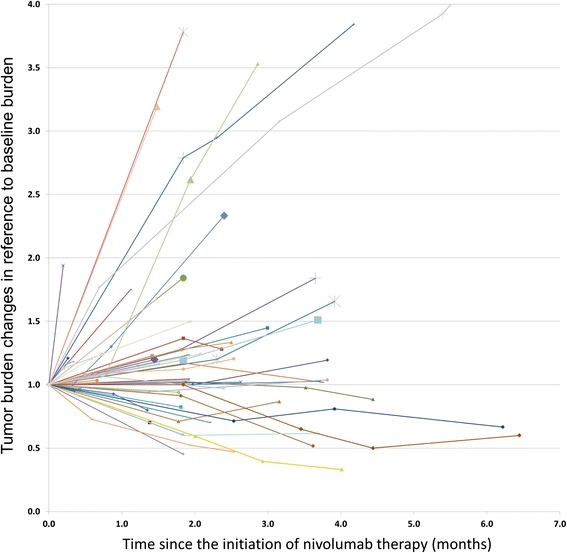
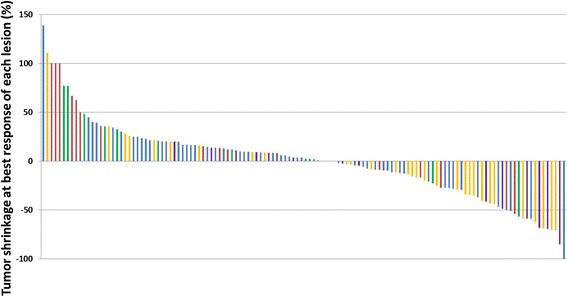
Tumor burden change at best overall response ranged from -66.8 to +278.1% (median: +3.9%). Response rate was 14% (8/56; 8 partial responses, 0 complete responses) by irRECIST1.1 and by RECIST1.1. Time-to-progression (TTP) by irRECIST1.1 was longer than TTP by RECIST1.1 (median TTP: not reached vs. 1.9 months, respectively). No patients experienced pseudoprogression during the study. Among 128 target lesions, the lesion-based size change at best response differed significantly across different organs, with adrenal lesions and lymph nodes having greater size decrease, followed by lung, while liver and other miscellaneous lesions had lesser degree of size decrease ( = 0.002).
Immune-related response evaluations using irRECIST1.1 in advanced NSCLC patients treated with nivolumab resulted in the identical response rate and longer TTP compared to RECIST1.1. No pseudoprogression cases were observed during the study. Adrenal lesions and lymph nodes were more responsive and liver lesions were less responsive to nivolumab.
在临床环境中,接受纳武单抗单药治疗的晚期非小细胞肺癌(NSCLC)患者使用免疫相关实体瘤疗效评价标准1.1(irRECIST1.1)的肿瘤反应特征此前尚未与根据传统实体瘤疗效评价标准1.1(RECIST1.1)进行的评估进行直接比较描述。
对56例在食品药品监督管理局(FDA)批准后接受纳武单抗单药治疗的晚期NSCLC患者进行回顾性研究。在治疗期间使用irRECIST1.1对系列CT扫描上的肿瘤负荷进行定量,irRECIST1.1采用一维测量并在总肿瘤负荷中纳入新病灶测量。将irRECIST1.1的反应评估与RECIST1.1的评估进行比较。还比较了不同器官中单个病灶的反应。
最佳总体反应时的肿瘤负荷变化范围为-66.8%至+278.1%(中位数:+3.9%)。irRECIST1.1和RECIST1.1的反应率均为14%(8/56;8例部分缓解,0例完全缓解)。irRECIST1.1的无进展生存期(TTP)长于RECIST1.1的TTP(中位数TTP:分别为未达到和1.9个月)。研究期间无患者经历假性进展。在128个靶病灶中,不同器官最佳反应时基于病灶的大小变化有显著差异,肾上腺病灶和淋巴结的大小减小更大,其次是肺部,而肝脏和其他杂类病灶的大小减小程度较小(=0.002)。
在接受纳武单抗治疗的晚期NSCLC患者中,使用irRECIST1.1进行免疫相关反应评估与RECIST1.1相比,反应率相同且TTP更长。研究期间未观察到假性进展病例。肾上腺病灶和淋巴结对纳武单抗反应更强,肝脏病灶反应较弱。