Aluisio Adam R, Teicher Carrei, Wiskel Tess, Guy Allysia, Levine Adam
Warren Alpert Medical School, Brown University, Providence, Rhode Island, USA.
Epicentre, Paris, France; Médecins Sans Frontières USA, New York, New York, USA.
PLoS Curr. 2016 Nov 16;8:ecurrents.dis.e75f9f9d977ac8adededb381e3948a04. doi: 10.1371/currents.dis.e75f9f9d977ac8adededb381e3948a04.
Lower extremity trauma during earthquakes accounts for the largest burden of geophysical disaster-related injuries. Insufficient pain management is common in disaster settings, and regional anesthesia (RA) has the potential to reduce pain in injured patients beyond current standards. To date, no prospective research has evaluated the use of RA in a disaster setting. This cross-sectional study assesses knowledge translation and skill acquisition outcomes for lower extremity RA performed with and without ultrasound guidance among a cohort of Médecins Sans Frontières (MSF) volunteers who will function as proceduralists in a planned randomized controlled trial evaluating the efficacy of RA for pain management in an earthquake setting.
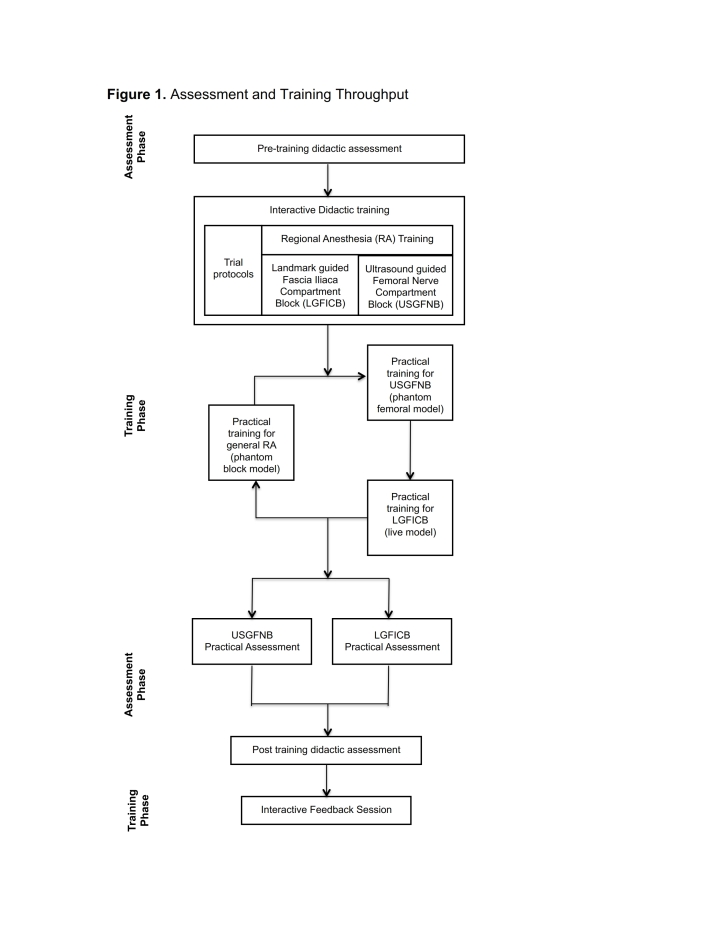
Generalist humanitarian healthcare responders, including both physicians and nurses, were trained in ultrasound guided femoral nerve block (USGFNB) and landmark guided fascia iliaca compartment block (LGFICB) techniques using didactic sessions and interactive simulations during a one-day focused course. Outcome measures evaluated interval knowledge attainment and technical proficiency in performing the RA procedures. Knowledge attainment was assessed via pre- and post-test evaluations and procedural proficiency was evaluated through monitored simulations, with performance of critical actions graded by two independent observers.
Twelve humanitarian response providers were enrolled and completed the trainings and assessments. Knowledge scores significantly increased from a mean pre-test score of 79% to post-test score of 88% (p<0.001). In practical evaluation of the LGFICB, participants correctly performed a median of 15.0 (Interquartile Range (IQR) 14.0-16.0) out of 16 critical actions. For the USGFNB, the median score was also 15.0 (IQR 14.0-16.0) out of 16 critical actions. Inter-rater reliability for completion of critical actions was excellent, with inter-rater agreement of 83.3% and 91.7% for the LGFICB and USGFNB evaluations, respectively.
Prior to conducting a trial of RA in a disaster setting, providers need to gain understanding and skills necessary to perform the interventions. This evaluation demonstrated attainment of high knowledge and technical skill scores in both physicians and nurses after a brief training in regional anesthesia techniques. This study demonstrates the feasibility of rapidly training generalist humanitarian responders to provide both LGFICB and USGFNB during humanitarian emergencies.
地震期间下肢创伤是与地球物理灾害相关损伤中负担最重的。在灾害环境中,疼痛管理不足很常见,而区域麻醉(RA)有可能减轻受伤患者的疼痛,超出当前标准。迄今为止,尚无前瞻性研究评估在灾害环境中使用RA的情况。这项横断面研究评估了在无国界医生组织(MSF)志愿者队列中,在有和没有超声引导的情况下进行下肢RA时的知识转化和技能习得结果,这些志愿者将在一项计划中的随机对照试验中担任手术医生,该试验旨在评估RA在地震环境中疼痛管理的疗效。
包括医生和护士在内的通才人道主义医疗响应者,在为期一天的集中课程中,通过理论授课和互动模拟,接受了超声引导股神经阻滞(USGFNB)和 landmark 引导髂筋膜间隙阻滞(LGFICB)技术的培训。结果指标评估了在进行RA手术过程中的知识获取间隔和技术熟练程度。知识获取通过课前和课后评估进行,手术熟练程度通过监测模拟进行评估,关键操作的表现由两名独立观察员评分。
招募了12名人道主义响应提供者并完成了培训和评估。知识得分从课前平均得分79%显著提高到课后得分88%(p<0.001)。在LGFICB的实际评估中,参与者在16项关键操作中正确完成的中位数为15.0(四分位间距(IQR)14.0 - 16.0)。对于USGFNB,在16项关键操作中的中位数得分也是15.0(IQR 14.0 - 16.0)。关键操作完成情况的评分者间信度极佳,LGFICB和USGFNB评估的评分者间一致性分别为83.3%和91.7%。
在灾害环境中进行RA试验之前,提供者需要获得进行干预所需的理解和技能。这项评估表明,在接受区域麻醉技术的简短培训后,医生和护士都获得了较高的知识和技术技能分数。本研究证明了快速培训通才人道主义响应者在人道主义紧急情况下提供LGFICB和USGFNB的可行性。