Sinha Indranil, Pusic Andrea L, Wilkins Edwin G, Hamill Jennifer B, Chen Xiaoxue, Kim Hyungjin M, Guldbrandsen Gretchen, Chun Yoon S
Boston, Mass.; New York, N.Y.; and Ann Arbor, Mich.
From the Division of Plastic Surgery, Brigham and Women's Hospital; the Division of Plastic and Reconstructive Surgery, Memorial Sloan Kettering Cancer Center; and the Section of Plastic Surgery and the Center for Statistical Consultation and Research, University of Michigan.
Plast Reconstr Surg. 2017 Jan;139(1):20-28. doi: 10.1097/PRS.0000000000002839.
Surgical-site infection causes devastating reconstructive failure in implant-based breast reconstructions. Large national database studies offer insights into complication rates, but only capture outcomes within 30 days postoperatively. This study evaluates both early and late surgical-site infection in immediate implant-based reconstruction and identifies predictors.
As part of the Mastectomy Reconstruction Outcomes Consortium Study, 1662 implant-based breast reconstructions in 1024 patients were evaluated for early versus late surgical-site infection. Early surgical-site infection was defined as infection occurring within 30 days postoperatively; late surgical-site infection was defined as infection occurring 31 days to 1 year postoperatively. Minor infection required oral antibiotics only, and major infection required hospitalization and/or surgical treatment. Direct-to-implant patients had 1-year follow-up, and tissue expander patients had 1-year post-exchange follow-up.
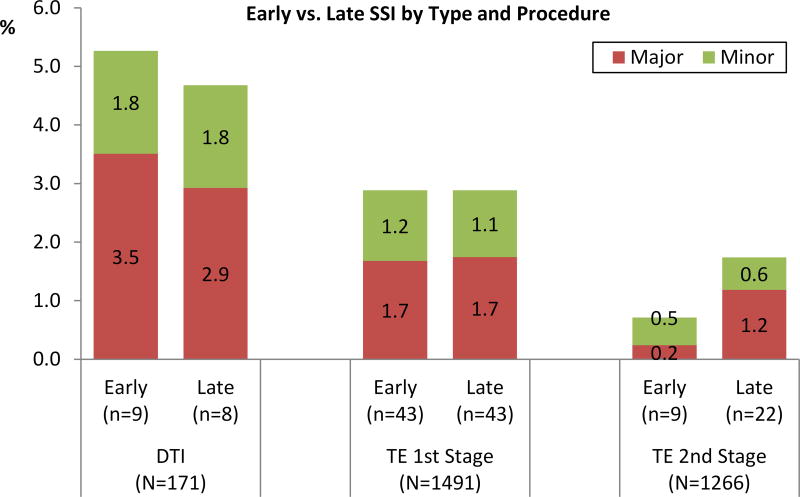
Among 1491 tissue expander and 171 direct-to-implant reconstructions, overall surgical-site infection rate for tissue expander was 5.7 percent (85 of 1491) after first-stage, 2.5 percent (31 of 1266) after second-stage, and 9.9 percent (17 of 171) for direct-to-implant reconstruction. Over 47 to 71 percent of surgical-site infection complications were late surgical-site infection. Multivariate analysis identified radiotherapy and increasing body mass index as significant predictors of late surgical-site infection. No significant difference between the direct-to-implant and tissue expander groups in the occurrence of early, late, or overall surgical-site infection was found.
The majority of surgical-site infection complications in immediate implant-based breast reconstructions occur more than 30 days after both first-stage and second-stage procedures. Radiotherapy and obesity are significantly associated with late-onset surgical-site infection. Current studies limited to early complications do not present a complete assessment of infection associated with implant-based breast reconstructions or their long-term clinical outcomes.
CLINICAL QUESTION/LEVEL OF EVIDENCE: Risk, II.
手术部位感染会导致基于植入物的乳房重建出现毁灭性的重建失败。大型全国性数据库研究提供了有关并发症发生率的见解,但仅记录术后30天内的结果。本研究评估即刻植入式重建中早期和晚期手术部位感染情况,并确定预测因素。
作为乳房切除术重建结果联盟研究的一部分,对1024例患者的1662例基于植入物的乳房重建进行了早期与晚期手术部位感染评估。早期手术部位感染定义为术后30天内发生的感染;晚期手术部位感染定义为术后31天至1年发生的感染。轻度感染仅需口服抗生素,重度感染则需要住院和/或手术治疗。直接植入式患者进行1年随访,组织扩张器患者在更换后进行1年随访。
在1491例组织扩张器和171例直接植入式重建中,组织扩张器第一阶段术后总体手术部位感染率为5.7%(1491例中的85例),第二阶段术后为2.5%(1266例中的31例),直接植入式重建为9.9%(171例中的17例)。超过47%至71%的手术部位感染并发症为晚期手术部位感染。多变量分析确定放疗和体重指数增加是晚期手术部位感染的重要预测因素。在早期、晚期或总体手术部位感染的发生率方面,直接植入式组和组织扩张器组之间未发现显著差异。
即刻植入式乳房重建中,大多数手术部位感染并发症发生在第一阶段和第二阶段手术后30天以上。放疗和肥胖与迟发性手术部位感染显著相关。目前仅限于早期并发症的研究并未对与基于植入物的乳房重建相关的感染及其长期临床结果进行全面评估。
临床问题/证据水平:风险,II级。