Kadota Tomohiro, Yano Tomonori, Kato Tomoji, Imajoh Maomi, Noguchi Masaaki, Morimoto Hiroyuki, Osera Shozo, Yoda Yusuke, Oono Yasuhiro, Ikematsu Hiroaki, Ohtsu Atsushi, Kaneko Kazuhiro
Department of Gastroenterology, Endoscopy Division, National Cancer Center Hospital East, Kashiwa, Chiba, Japan; Course of Advanced Clinical Research of Cancer, Juntendo University Graduate School of Medicine, Tokyo, Japan.
Department of Gastroenterology, Endoscopy Division, National Cancer Center Hospital East, Kashiwa, Chiba, Japan.
Endosc Int Open. 2016 Dec;4(12):E1267-E1274. doi: 10.1055/s-0042-118291. Epub 2016 Nov 21.
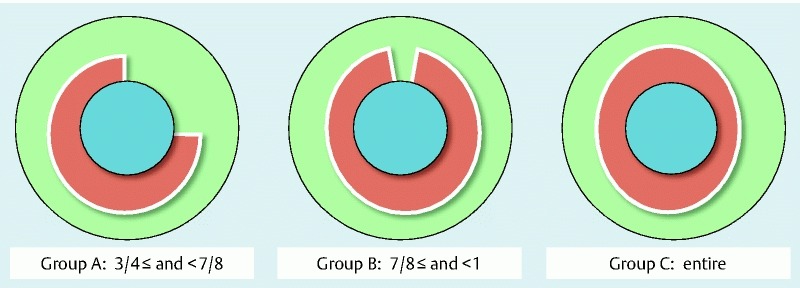
One of the major complications after endoscopic resection (ER) for large superficial esophageal squamous cell carcinoma (ESCC) is benign esophageal stricture, which can reduce quality of life even if ESCC achieves a cure without organ resection. Recently, steroid administration has been reported as a prophylactic treatment to prevent esophageal strictures. This retrospective study evaluated the stricture rate according to the different width of mucosal defects due to ER and compared it to that seen with prophylactic steroid administration. Between June 2007 and December 2013, we enrolled patients with ESCC who had 3/4 or larger circumferential mucosal defects due to ER. In December 2009, steroid injections (triamcinolone acetonide 50 mg) into the ulcer bed due to ER were introduced. Beginning in November 2012, we commenced oral steroid administration (prednisolone 30 mg/day, tapered gradually for 8 weeks) in addition to steroid injection. Patients were classified into 3 groups according to the width of mucosal defect after ER (Group A, ≥ 3/4 and < 7/8; Group B, ≥ 7/8 and less than the entire circumference; and Group C, the entire circumference). We retrospectively evaluated the stricture rate by comparing no treatment, steroid injection, or steroid injection followed by oral steroid according to the width of mucosal defect. A total of 115 patients met the selection criteria. In Group B, no treatment had a significantly higher stricture rate (100 %, vs. steroid injection: 56 % = 0.015; vs steroid injection followed by oral steroid: 20 % < 0.001). Conversely, in Group C, the stricture rate was high, regardless of treatment (no treatment: 100 %; steroid injection: 100 %; steroid injection followed by oral steroid: 71 %). Although prophylactic steroid administration is effective to prevent strictures for 7/8 circumference or larger mucosal defects, it is ineffective for whole-circumference defects. Further investigation is required.
内镜下切除(ER)治疗大型浅表性食管鳞状细胞癌(ESCC)后的主要并发症之一是良性食管狭窄,即使ESCC在未进行器官切除的情况下实现治愈,也会降低生活质量。最近,有报道称给予类固醇作为预防食管狭窄的治疗方法。这项回顾性研究根据ER导致的黏膜缺损不同宽度评估了狭窄率,并将其与预防性使用类固醇治疗的狭窄率进行比较。2007年6月至2013年12月,我们纳入了因ER导致3/4或更大圆周黏膜缺损的ESCC患者。2009年12月,开始对ER导致的溃疡床注射类固醇(曲安奈德50mg)。从2012年11月起,除注射类固醇外,我们还开始口服类固醇(泼尼松龙30mg/天,逐渐减量,持续8周)。根据ER后黏膜缺损的宽度将患者分为3组(A组,≥3/4且<7/8;B组,≥7/8且小于整个圆周;C组,整个圆周)。我们通过比较根据黏膜缺损宽度进行的无治疗、类固醇注射或类固醇注射后口服类固醇的情况,回顾性评估狭窄率。共有115例患者符合入选标准。在B组中,无治疗的狭窄率显著更高(100%,与类固醇注射相比:56%,P = 0.015;与类固醇注射后口服类固醇相比:20%,P < 0.001)。相反,在C组中,无论何种治疗,狭窄率都很高(无治疗:100%;类固醇注射:100%;类固醇注射后口服类固醇:71%)。尽管预防性使用类固醇对预防7/8圆周或更大的黏膜缺损狭窄有效,但对全圆周缺损无效。需要进一步研究。