Zhang Ruyang, Wang Zhaoxi, Tejera Paula, Frank Angela J, Wei Yongyue, Su Li, Zhu Zhaozhong, Guo Yichen, Chen Feng, Bajwa Ednan K, Thompson B Taylor, Christiani David C
Department of Environmental Health, Harvard School of Public Health, Pulmonary and Critical Care Division, Department of Medicine, Massachusetts General Hospital and Harvard Medical School, 665 Hunting Avenue, Building I Room 1401, Boston, MA, 02115, USA.
Department of Biostatistics, Ministry of Education Key Laboratory for Modern Toxicology, School of Public Health, Nanjing Medical University, Nanjing, China.
Intensive Care Med. 2017 Mar;43(3):399-407. doi: 10.1007/s00134-016-4638-3. Epub 2016 Dec 28.
To evaluate the association between acute respiratory distress syndrome (ARDS) onset time and prognosis.
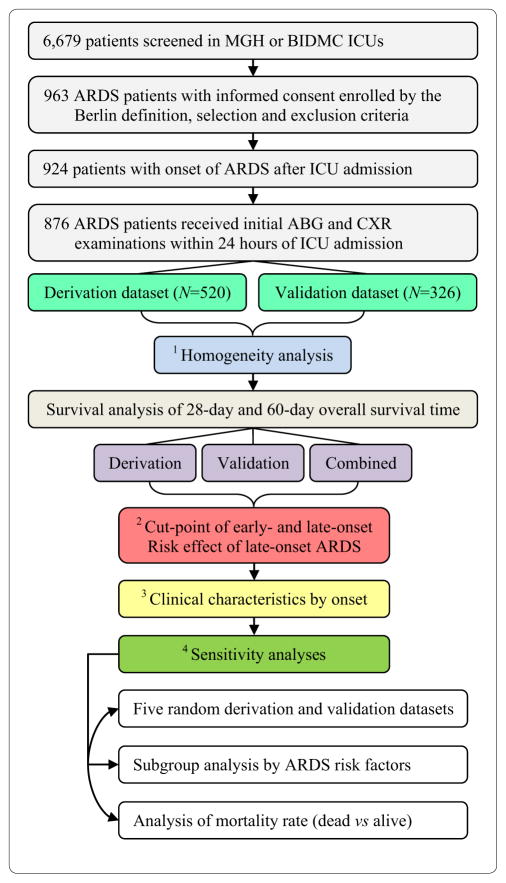
Patients with moderate to severe ARDS (N = 876) were randomly assigned into derivation (N = 520) and validation (N = 356) datasets. Both 28-day and 60-day survival times after ARDS onset were analyzed. A data-driven cutoff point between early- and late-onset ARDS was determined on the basis of mortality risk effects of onset times. We estimated the hazard ratio (HR) and odds ratio (OR) of late-onset ARDS using a multivariate Cox proportional hazards model of survival time and a multivariate logistic regression model of mortality rate, respectively.
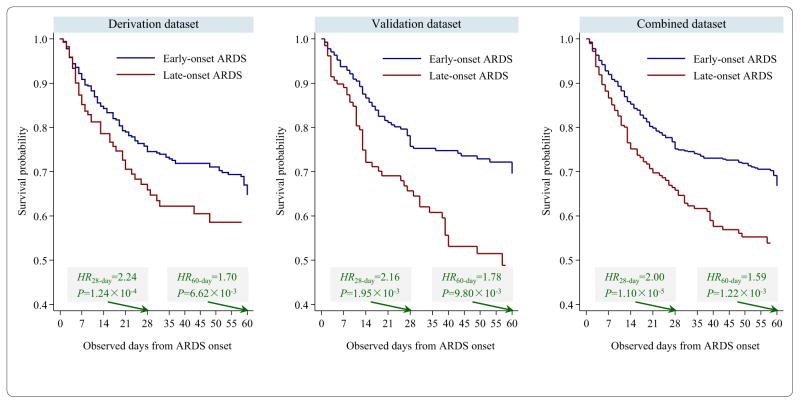
Late-onset ARDS, defined as onset over 48 h after intensive care unit (ICU) admission (N = 273, 31%), was associated with shorter 28-day survival time: HR = 2.24, 95% CI 1.48-3.39, P = 1.24 × 10 (derivation); HR = 2.16, 95% CI 1.33-3.51, P = 1.95 × 10 (validation); and HR = 2.00, 95% CI 1.47-2.72, P = 1.10 × 10 (combined dataset). Late-onset ARDS was also associated with shorter 60-day survival time: HR = 1.70, 95% CI 1.16-2.48, P = 6.62 × 10 (derivation); HR = 1.78, 95% CI 1.15-2.75, P = 9.80 × 10 (validation); and HR = 1.59, 95% CI 1.20-2.10, P = 1.22 × 10 (combined dataset). Meanwhile, late-onset ARDS was associated with higher 28-day mortality rate (OR = 1.46, 95% CI 1.04-2.06, P = 0.0305) and 60-day mortality rate (OR = 1.44, 95% CI 1.03-2.02, P = 0.0313).
Late-onset moderate to severe ARDS patients had both shorter survival time and higher mortality rate in 28-day and 60-day observations.
评估急性呼吸窘迫综合征(ARDS)发病时间与预后之间的关联。
将中度至重度ARDS患者(N = 876)随机分为推导数据集(N = 520)和验证数据集(N = 356)。分析ARDS发病后28天和60天的生存时间。根据发病时间的死亡风险效应确定早发性和迟发性ARDS之间的数据驱动截断点。我们分别使用生存时间的多变量Cox比例风险模型和死亡率的多变量逻辑回归模型估计迟发性ARDS的风险比(HR)和比值比(OR)。
迟发性ARDS定义为重症监护病房(ICU)入院后48小时以上发病(N = 273,31%),与28天生存时间较短相关:HR = 2.24,95% CI 1.48 - 3.39,P = 1.24×10(推导数据集);HR = 2.16,95% CI 1.33 - 3.51,P = 1.95×10(验证数据集);HR = 2.00,95% CI 1.47 - 2.72,P = 1.10×10(合并数据集)。迟发性ARDS也与60天生存时间较短相关:HR = 1.70,95% CI 1.16 - 2.48,P = 6.62×10(推导数据集);HR = 1.78,95% CI 1.15 - 2.75,P = 9.80×10(验证数据集);HR = 1.59,95% CI 1.20 - 2.10,P = 1.22×10(合并数据集)。同时,迟发性ARDS与28天死亡率较高(OR = 1.46,95% CI 1.04 - 2.06,P = 0.0305)和60天死亡率较高(OR = 1.44,95% CI 1.03 - 2.02,P = 0.0313)相关。
在28天和60天的观察中,迟发性中度至重度ARDS患者的生存时间较短且死亡率较高。