Lyberg Katarina, Ali Hani Abdulkadir, Grootens Jennine, Kjellander Matilda, Tirfing Malin, Arock Michel, Hägglund Hans, Nilsson Gunnar, Ungerstedt Johanna
Immunology and Allergy Unit, Department of Medicine Solna, Karolinska Institutet and clinical immunology and transfusion medicine, Karolinska University Hospital, Stockholm, Sweden.
Mastocytosis Center Karolinska, Karolinska University Hospital and Karolinska Institutet, Stockholm, Sweden.
Oncotarget. 2017 Feb 7;8(6):9647-9659. doi: 10.18632/oncotarget.14181.
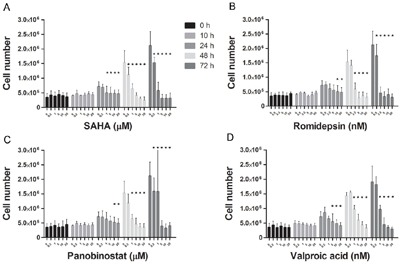
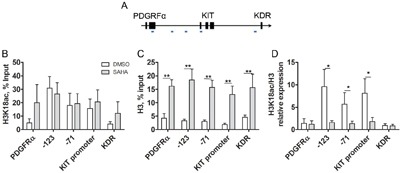
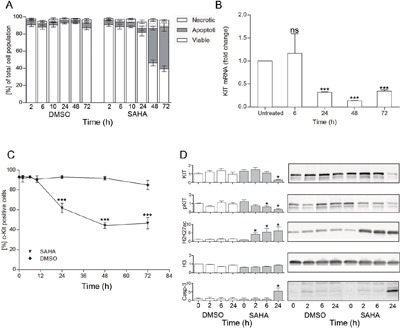
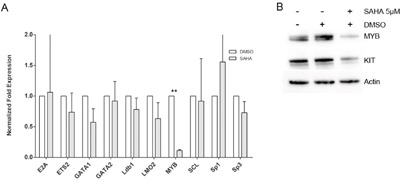
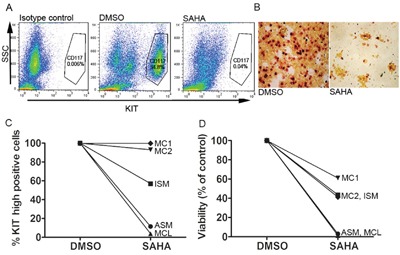
Systemic mastocytosis (SM) is a clonal bone marrow disorder, where therapeutical options are limited. Over 90% of the patients carry the D816V point mutation in the KIT receptor that renders this receptor constitutively active. We assessed the sensitivity of primary mast cells (MC) and mast cell lines HMC1.2 (D816V mutated), ROSA (KIT WT) and ROSA (KIT D816V) cells to histone deacetylase inhibitor (HDACi) treatment. We found that of four HDACi, suberoyl anilide hydroxamic acid (SAHA) was the most effective in killing mutated MC. SAHA downregulated KIT, followed by major MC apoptosis. Primary SM patient MC cultured ex vivo were even more sensitive to SAHA than HMC1.2 cells, whereas primary MC from healthy subjects were less affected. There was a correlation between cell death and SM disease severity, where cell death was more pronounced in the case of aggressive SM, with almost 100% cell death among MC from the mast cell leukemia patient. Additionally, ROSA (KIT D816V) was more affected by HDACi than ROSA (KIT WT) cells. Using ChIP qPCR, we found that the level of active chromatin mark H3K18ac/H3 decreased significantly in the KIT region. This epigenetic silencing was seen only in the KIT region and not in control genes upstream and downstream of KIT, indicating that the downregulation of KIT is exerted by specific epigenetic silencing. In conclusion, KIT D816V mutation sensitized MC to HDACi mediated killing, and SAHA may be of value as specific treatment for SM, although the specific mechanism of action requires further investigation.
系统性肥大细胞增多症(SM)是一种克隆性骨髓疾病,其治疗选择有限。超过90%的患者在KIT受体中携带D816V点突变,该突变使该受体持续激活。我们评估了原代肥大细胞(MC)以及肥大细胞系HMC1.2(D816V突变型)、ROSA(KIT野生型)和ROSA(KIT D816V)细胞对组蛋白去乙酰化酶抑制剂(HDACi)治疗的敏感性。我们发现,在四种HDACi中,辛二酰苯胺异羟肟酸(SAHA)在杀死突变型MC方面最有效。SAHA下调KIT,随后导致主要的MC凋亡。体外培养的原发性SM患者MC对SAHA甚至比HMC1.2细胞更敏感,而健康受试者的原代MC受影响较小。细胞死亡与SM疾病严重程度之间存在相关性,在侵袭性SM病例中细胞死亡更为明显,肥大细胞白血病患者的MC中几乎100%细胞死亡。此外,ROSA(KIT D816V)比ROSA(KIT野生型)细胞受HDACi的影响更大。使用染色质免疫沉淀定量PCR(ChIP qPCR),我们发现KIT区域中活性染色质标记H3K18ac/H3的水平显著降低。这种表观遗传沉默仅在KIT区域出现,而在KIT上游和下游的对照基因中未出现,这表明KIT的下调是由特定的表观遗传沉默所导致。总之,KIT D816V突变使MC对HDACi介导的杀伤敏感,SAHA可能作为SM的特异性治疗具有价值,尽管其具体作用机制需要进一步研究。