Bulluck Heerajnarain, Nicholas Jennifer, Crimi Gabriele, White Steven K, Ludman Andrew J, Pica Silvia, Raineri Claudia, Cabrera-Fuentes Hector A, Yellon Derek, Rodriguez-Palomares Jose, Garcia-Dorado David, Hausenloy Derek J
The Hatter Cardiovascular Institute, Institute of Cardiovascular Science, University College London, UK; The National Institute of Health Research University College London Hospitals Biomedical Research Centre, UK; National Heart Research Institute Singapore, National Heart Centre Singapore, Singapore.
London School Hygiene and Tropical Medicine, London, UK.
Int J Cardiol. 2017 Mar 1;230:149-154. doi: 10.1016/j.ijcard.2016.12.030. Epub 2016 Dec 19.
Clinical studies using serum cardiac biomarkers to investigate a circadian variation in acute myocardial infarct (MI) size in ST-segment elevation myocardial infarction (STEMI) patients reperfused by primary percutaneous coronary intervention (PPCI) have produced mixed results. We aimed to investigate this phenomenon using acute MI size measured by cardiovascular magnetic resonance (CMR).
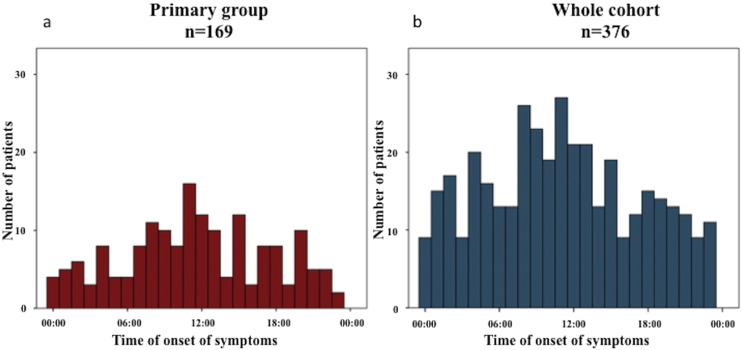
Patient-level data was obtained from 4 randomized controlled trials investigating the MI-limiting effects of cardioprotective therapies in this pooled analysis. The primary analysis was performed in those patients with no pre-infarct angina; duration of ischemia >60min and <360min; Thrombolysis In Myocardial Infarction (TIMI) flow pre-PPCI ≤1; TIMI flow post-PPCI 3; and no collateral flow.
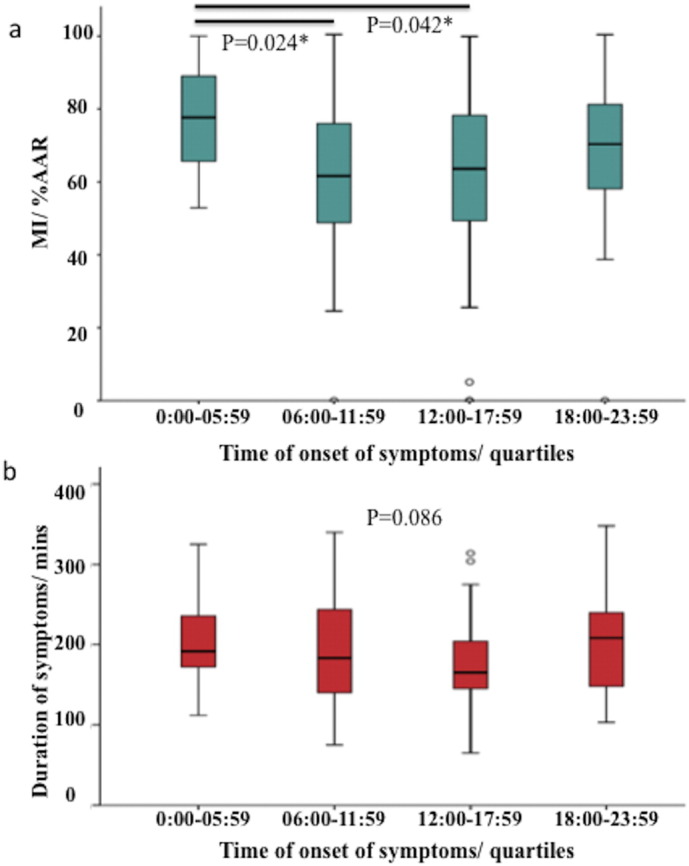
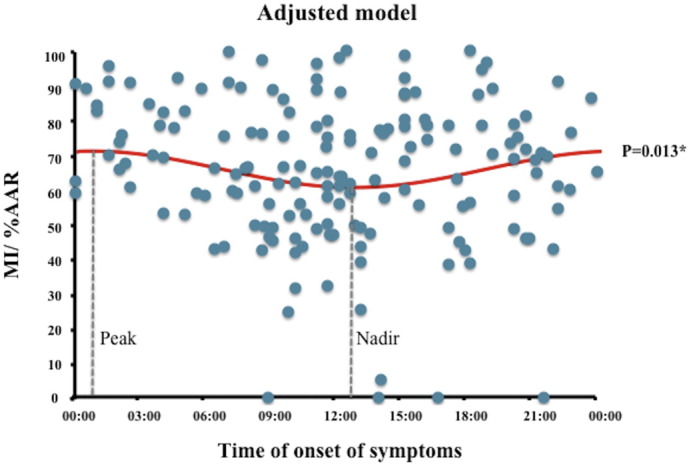
169 out of 376 patients with CMR data met the inclusion criteria for the primary analysis. A 24-hour circadian variation in acute MI size as a % of the area-at-risk (%AAR), after adjusting for confounders, was observed with a peak and nadir MI size in patients with symptom onset between 00:00 and 01:00 and between 12:00 and 13:00 respectively (difference from the average MI size 5.2%, 95%CI 1.1-9.4%; p=0.013). This was associated with a non-significant circadian variation in left ventricular ejection fraction (LVEF) (difference from the average LVEF 5.9%, 95%CI -0.6-2.2%, p=0.073). There was no circadian variation in MI size or LVEF in the whole cohort.
We report a circadian variation in acute MI size assessed by CMR in a subset of STEMI patients treated by PPCI, with the largest and smallest MI size occurring in patients with symptom onset between 00:00 and 01:00 and between 12:00 and 13:00 respectively.
利用血清心脏生物标志物研究接受直接经皮冠状动脉介入治疗(PPCI)再灌注的ST段抬高型心肌梗死(STEMI)患者急性心肌梗死(MI)面积的昼夜变化的临床研究结果不一。我们旨在通过心血管磁共振(CMR)测量的急性MI面积来研究这一现象。
在这项汇总分析中,患者水平的数据来自4项研究心脏保护疗法对MI限制作用的随机对照试验。对那些无梗死前心绞痛;缺血持续时间>60分钟且<360分钟;PPCI前心肌梗死溶栓(TIMI)血流≤1;PPCI后TIMI血流3;且无侧支血流的患者进行了初步分析。
376例有CMR数据的患者中,169例符合初步分析的纳入标准。在调整混杂因素后,观察到急性MI面积占危险区域面积的百分比(%AAR)存在24小时的昼夜变化,症状发作时间在00:00至01:00之间和12:00至13:00之间的患者,MI面积分别达到峰值和最低点(与平均MI面积的差异为5.2%,95%CI 1.1 - 9.4%;p = 0.013)。这与左心室射血分数(LVEF)的昼夜变化无显著相关性(与平均LVEF的差异为5.9%,95%CI - 0.6 - 2.2%,p = 0.073)。整个队列中MI面积或LVEF无昼夜变化。
我们报告了在接受PPCI治疗的STEMI患者亚组中,通过CMR评估的急性MI面积存在昼夜变化,症状发作时间在00:00至01:00之间和12:00至13:00之间的患者,MI面积分别最大和最小。