Markar S R, Noordman B J, Mackenzie H, Findlay J M, Boshier P R, Ni M, Steyerberg E W, van der Gaast A, Hulshof M C C M, Maynard N, van Berge Henegouwen M I, Wijnhoven B P L, Reynolds J V, Van Lanschot J J B, Hanna G B
Department of Surgery & Cancer, Imperial College London, London, UK.
Department of Surgery, Erasmus MC-University Medical Centre, Rotterdam, Netherlands.
Ann Oncol. 2017 Mar 1;28(3):519-527. doi: 10.1093/annonc/mdw560.
The primary aim of this study was to compare survival from neoadjuvant chemoradiotherapy plus surgery (NCRS) versus neoadjuvant chemotherapy plus surgery (NCS) for the treatment of esophageal or junctional adenocarcinoma. The secondary aims were to compare pathological effects, short-term mortality and morbidity, and to evaluate the effect of lymph node harvest upon survival in both treatment groups.
Data were collected from 10 European centers from 2001 to 2012. Six hundred and eight patients with stage II or III oesophageal or oesophago-gastric junctional adenocarcinoma were included; 301 in the NCRS group and 307 in the NCS group. Propensity score matching and Cox regression analyses were used to compensate for differences in baseline characteristics.
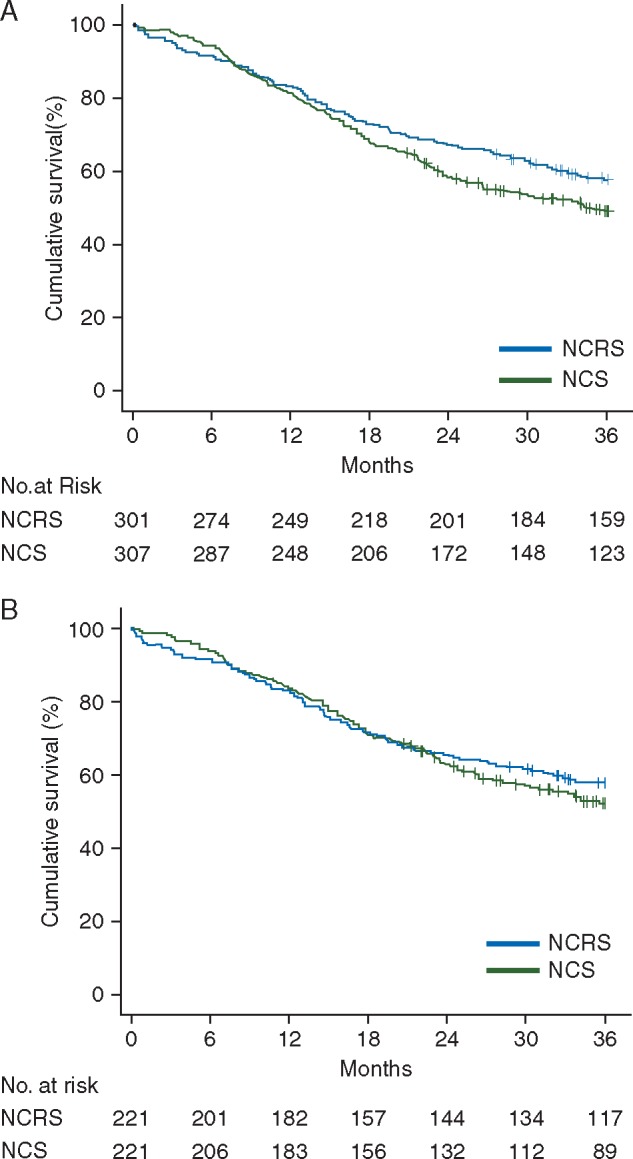
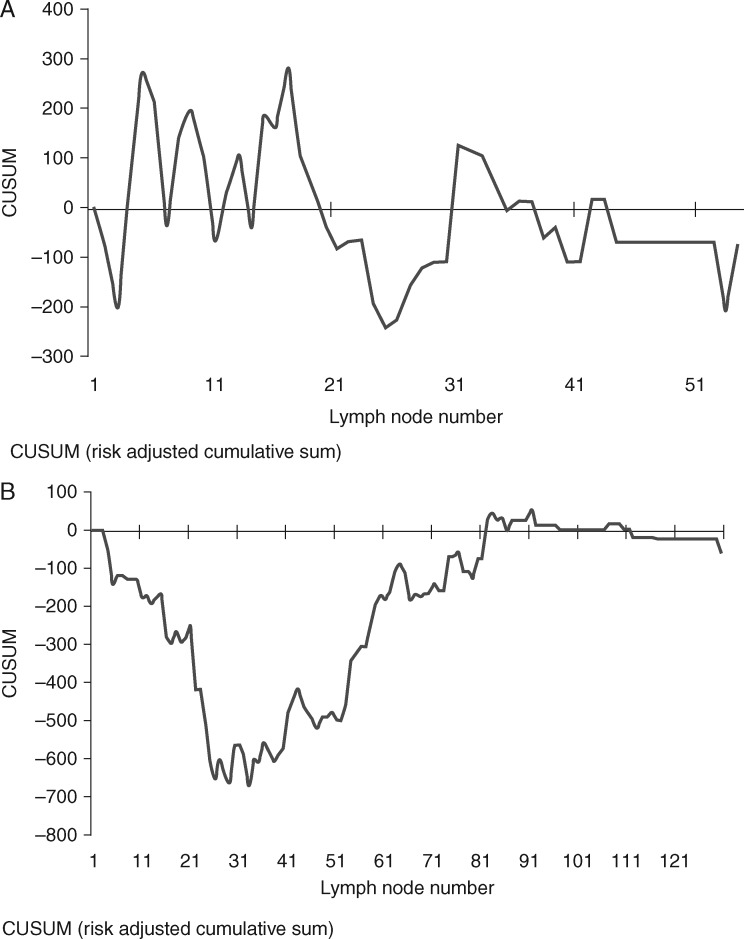
NCRS resulted in significant pathological benefits with more ypT0 (26.7% versus 5%; P < 0.001), more ypN0 (63.3% versus 32.1%; P < 0.001), and reduced R1/2 resection margins (7.7% versus 21.8%; P < 0.001). Analysis of short-term outcomes showed no statistically significant differences in 30-day or 90-day mortality, but increased incidence of anastomotic leak (23.1% versus 6.8%; P < 0.001) in NCRS patients. There were no statistically significant differences between the groups in 3-year overall survival (57.9% versus 53.4%; Hazard Ratio (HR)= 0.89, 95%C.I. 0.67-1.17, P = 0.391) nor disease-free survival (52.9% versus 48.9%; HR = 0.90, 95%C.I. 0.69-1.18, P = 0.443). The pattern of recurrence was also similar (P = 0.660). There was a higher lymph node harvest in the NCS group (27 versus 14; P < 0.001), which was significantly associated with a lower recurrence rate and improved disease free survival within the NCS group.
The survival differences between NCRS and NCS maybe modest, if present at all, for the treatment of locally advanced esophageal or junctional adenocarcinoma. Future large-scale randomized trials must control and monitor indicators of the quality of surgery, as the extent of lymphadenectomy appears to influence prognosis in patients treated with NCS, from this large multi-center European study.
本研究的主要目的是比较新辅助放化疗联合手术(NCRS)与新辅助化疗联合手术(NCS)治疗食管或食管胃交界腺癌的生存率。次要目的是比较病理疗效、短期死亡率和发病率,并评估两组中淋巴结清扫对生存的影响。
收集了2001年至2012年来自10个欧洲中心的数据。纳入608例II期或III期食管或食管胃交界腺癌患者;NCRS组301例,NCS组307例。采用倾向评分匹配和Cox回归分析来弥补基线特征的差异。
NCRS带来了显著的病理益处,ypT0更多(26.7%对5%;P<0.001),ypN0更多(63.3%对32.1%;P<0.001),R1/2切缘减少(7.7%对21.8%;P<0.001)。短期结果分析显示,30天或90天死亡率无统计学显著差异,但NCRS患者吻合口漏发生率增加(23.1%对6.8%;P<0.001)。两组在3年总生存率(57.9%对53.4%;风险比(HR)=0.89,95%置信区间0.67-1.17,P=0.391)和无病生存率(52.9%对48.9%;HR=0.90,95%置信区间0.69-1.18,P=0.443)方面均无统计学显著差异。复发模式也相似(P=0.660)。NCS组的淋巴结清扫数量更多(27个对14个;P<0.001),这与NCS组较低的复发率和改善的无病生存率显著相关。
对于局部晚期食管或食管胃交界腺癌的治疗,NCRS和NCS之间的生存差异可能不大,即便存在差异。从这项大型多中心欧洲研究来看,由于淋巴结清扫范围似乎会影响接受NCS治疗患者的预后,未来的大规模随机试验必须控制和监测手术质量指标。