Hori Tomohide, Kaido Toshimi, Iida Taku, Yagi Shintaro, Uemoto Shinji
Department of Hepatobiliary Pancreatic and Transplant Surgery, Kyoto University Hospital, Kyoto, Japan.
Ann Gastroenterol. 2017;30(1):118-126. doi: 10.20524/aog.2016.0088. Epub 2016 Sep 22.
A living donor (LD) for liver transplantation (LT) is the best target for minimally invasive surgery. Laparoscope-assisted surgery (LAS) for LDs has gradually evolved. A donor safety rate of 100% should be guaranteed.
We began performing LAS for LDs in June 2012. The aim of this report is to describe the surgical procedures of LAS in detail, discuss various tips and pitfalls, and address the potential for a smooth transition to more advanced LAS.
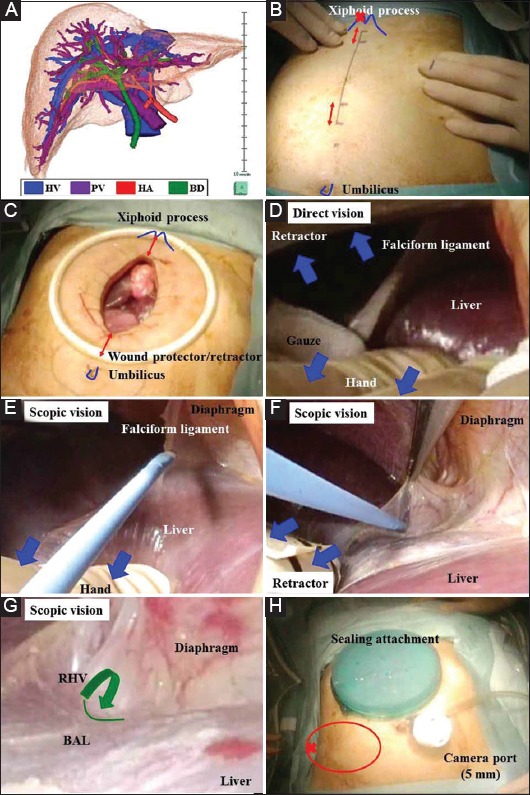
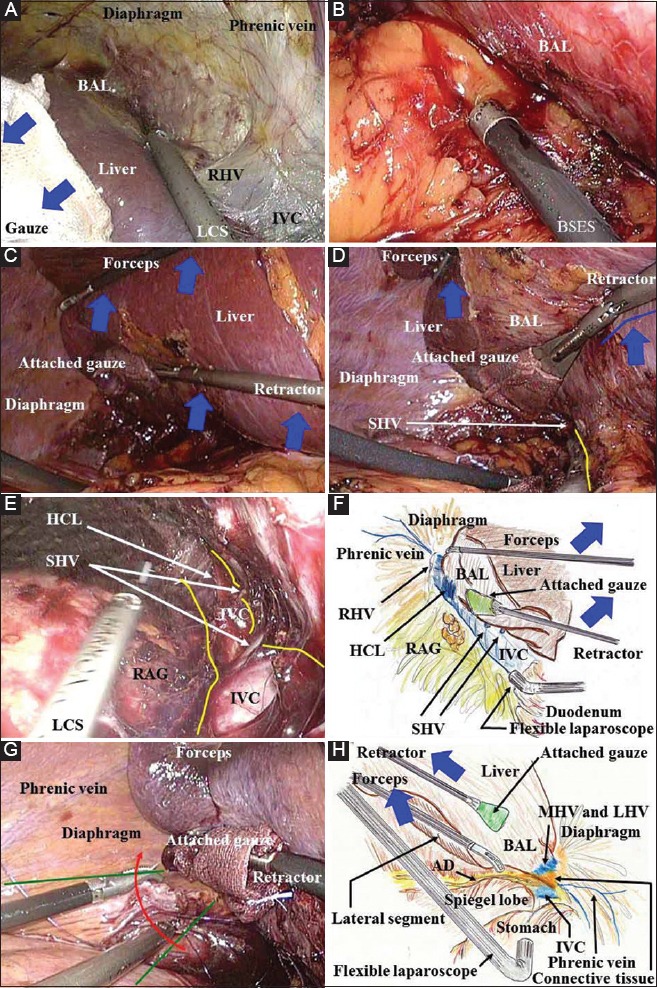
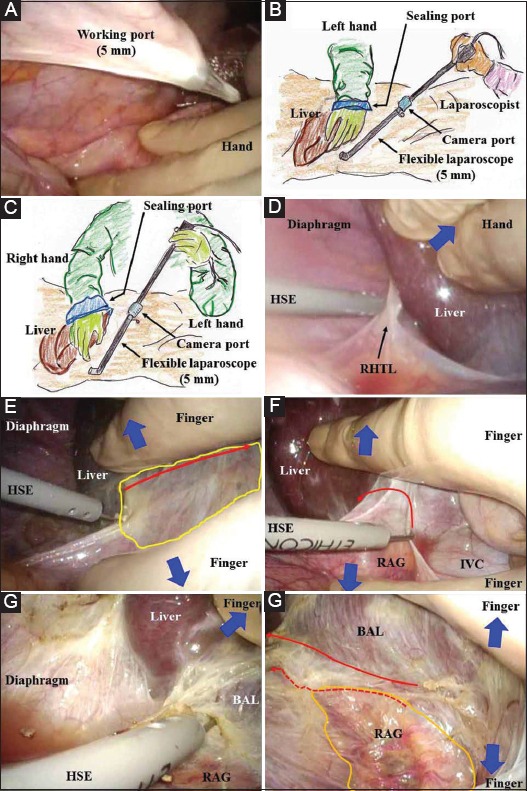
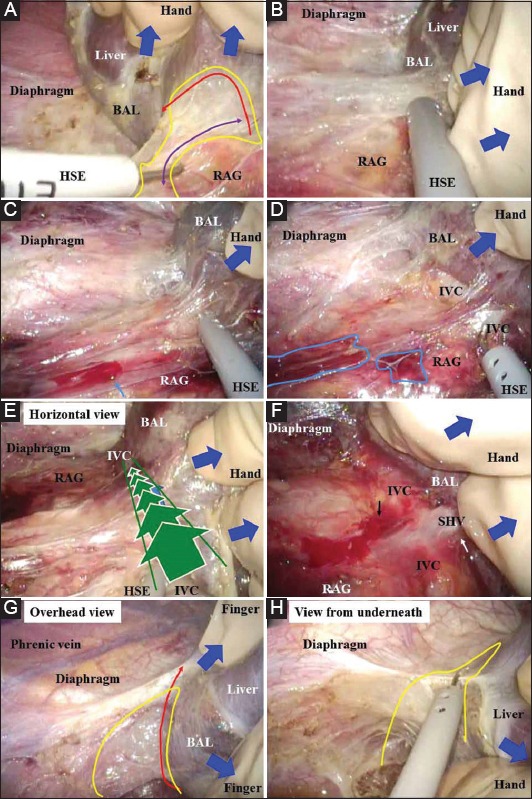
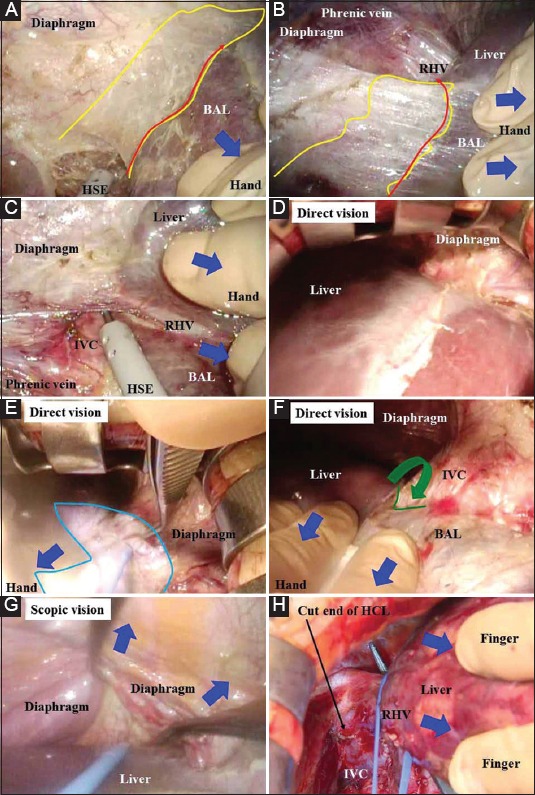
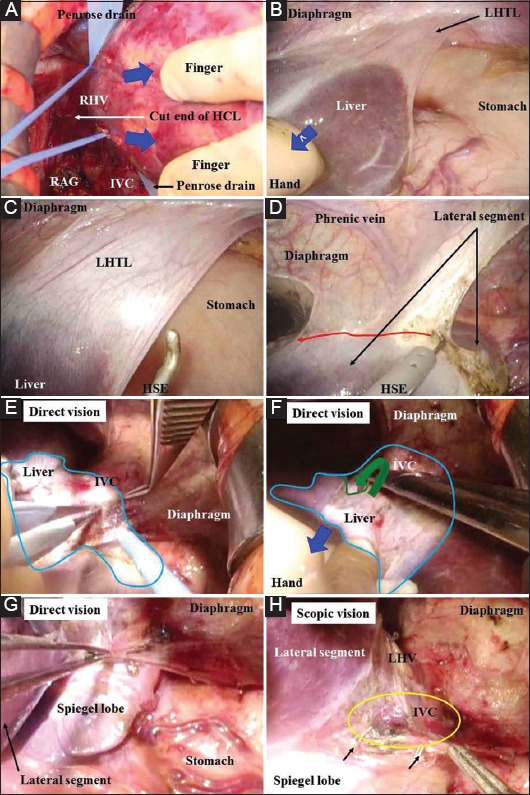
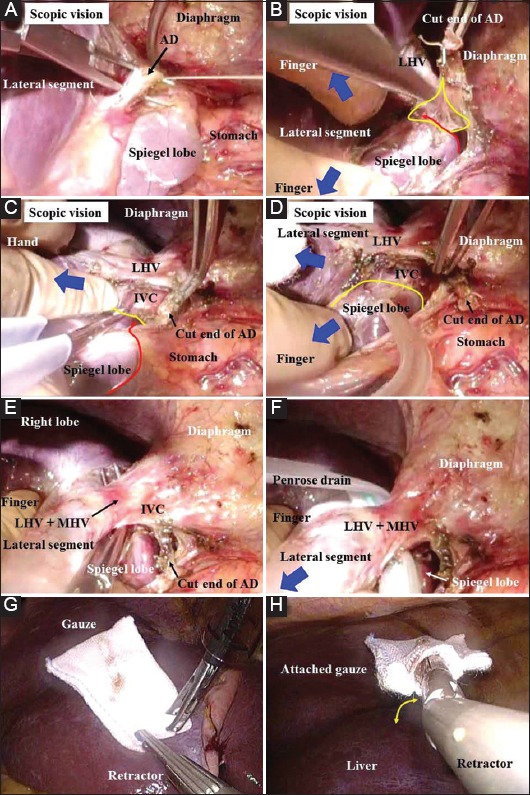
Preoperative planning based on three-dimensional image analysis is a powerful tool for successful surgery. The combination of liver retraction/countertraction and the pressure produced by pneumoperitoneum widens the dissectible/cuttable layer, increasing the safety of LAS. A flexible laparoscope provides excellent magnified vision in both the horizontal view along the inferior vena cava, under adequate liver retraction, and in the lateral view, to harvest left-sided grafts in critical procedures. Intentional omission of painful incisions is beneficial for LDs. Hepatectomy using a smaller midline incision is safe if a hanging maneuver is used. Safe transition from LAS to a hybrid technique involving a combination of pure laparoscopic surgery and subsequent open surgery seems possible.
LDLT surgeons have a very broad intellectual and technical frontier.
肝移植活体供体(LD)是微创手术的最佳目标。针对LD的腹腔镜辅助手术(LAS)已逐渐发展。应确保供体安全率达到100%。
我们于2012年6月开始对LD实施LAS。本报告旨在详细描述LAS的手术步骤,讨论各种技巧和陷阱,并探讨顺利过渡到更先进LAS的可能性。
基于三维图像分析的术前规划是成功手术的有力工具。肝脏牵拉/反向牵拉与气腹产生的压力相结合,拓宽了可解剖/可切割层面,提高了LAS的安全性。在充分牵拉肝脏的情况下,柔性腹腔镜在沿下腔静脉的水平视野以及在侧视野中均能提供出色的放大视野,以便在关键步骤中获取左侧供肝。有意省略疼痛切口对LD有益。如果采用悬吊手法,使用较小的中线切口进行肝切除术是安全的。从LAS顺利过渡到涉及单纯腹腔镜手术及后续开放手术相结合的混合技术似乎是可行的。
活体肝移植外科医生面临着非常广阔的知识和技术前沿。