Lee Ji Won, Lim Do Hoon, Sung Ki Woong, Lee Hyeong Jin, Yi Eun Sang, Yoo Keon Hee, Koo Hong Hoe, Suh Yeon Lim, Shin Hyung Jin
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
J Korean Med Sci. 2017 Feb;32(2):195-203. doi: 10.3346/jkms.2017.32.2.195.
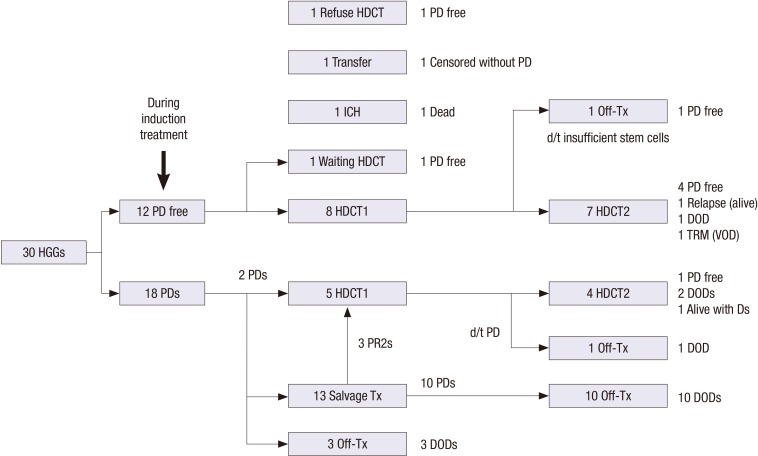
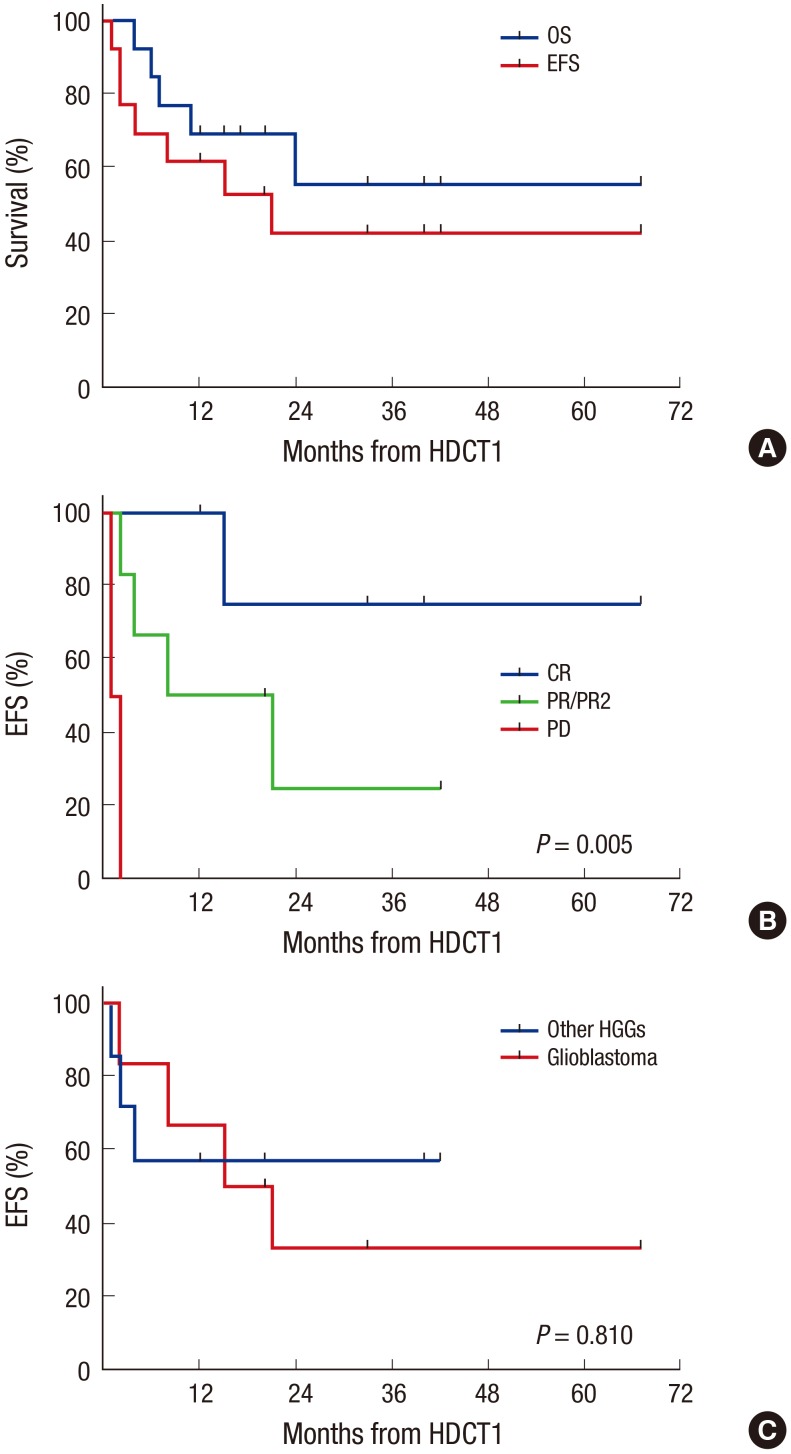
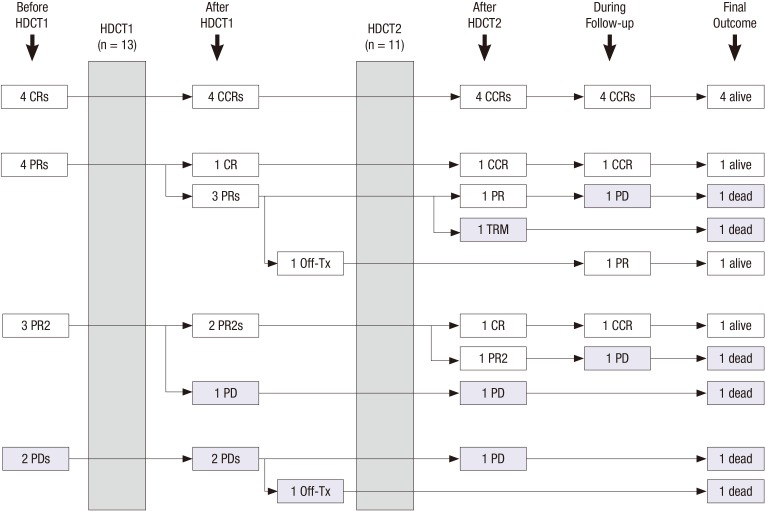
With the aim to investigate the outcome of tandem high-dose chemotherapy and autologous stem cell transplantation (HDCT/auto-SCT) for high-grade gliomas (HGGs), we retrospectively reviewed the medical records of 30 patients with HGGs (16 glioblastomas, 7 anaplastic astrocytomas, and 7 other HGGs) between 2006 and 2015. Gross or near total resection was possible in 11 patients. Front-line treatment after surgery was radiotherapy (RT) in 14 patients and chemotherapy in the remaining 16 patients including 3 patients less than 3 years of age. Eight of 12 patients who remained progression free and 5 of the remaining 18 patients who experienced progression during induction treatment underwent the first HDCT/auto-SCT with carboplatin + thiotepa + etoposide (CTE) regimen and 11 of them proceeded to the second HDCT/auto-SCT with cyclophosphamide + melphalan (CyM) regimen. One patient died from hepatic veno-occlusive disease (VOD) during the second HDCT/auto-SCT; otherwise, toxicities were manageable. Four patients in complete response (CR) and 3 of 7 patients in partial response (PR) or second PR at the first HDCT/auto-SCT remained event free: however, 2 patients with progressive tumor experienced progression again. The probabilities of 3-year overall survival (OS) after the first HDCT/auto-SCT in 11 patients in CR, PR, or second PR was 58.2% ± 16.9%. Tumor status at the first HDCT/auto-SCT was the only significant factor for outcome after HDCT/auto-SCT. There was no difference in survival between glioblastoma and other HGGs. This study suggests that the outcome of HGGs in children and adolescents after HDCT/auto-SCT is encouraging if the patient could achieve CR or PR before HDCT/auto-SCT.
为了研究串联大剂量化疗及自体干细胞移植(HDCT/auto-SCT)治疗高级别胶质瘤(HGG)的疗效,我们回顾性分析了2006年至2015年间30例HGG患者(16例胶质母细胞瘤、7例间变性星形细胞瘤和7例其他HGG)的病历。11例患者可行肉眼或近全切手术。术后一线治疗中,14例患者接受放疗(RT),其余16例患者接受化疗,其中包括3例年龄小于3岁的患者。诱导治疗期间无进展的12例患者中的8例以及进展的其余18例患者中的5例接受了首次HDCT/auto-SCT,采用卡铂+噻替派+依托泊苷(CTE)方案,其中11例继续接受第二次HDCT/auto-SCT,采用环磷酰胺+美法仑(CyM)方案。1例患者在第二次HDCT/auto-SCT期间死于肝静脉闭塞病(VOD);除此之外,毒性反应可控。首次HDCT/auto-SCT时4例完全缓解(CR)患者以及7例部分缓解(PR)或第二次PR患者中的3例无事件发生:然而,2例肿瘤进展患者再次出现进展。11例CR、PR或第二次PR患者首次HDCT/auto-SCT后3年总生存(OS)率为58.2%±16.9%。首次HDCT/auto-SCT时的肿瘤状态是HDCT/auto-SCT后疗效的唯一显著因素。胶质母细胞瘤与其他HGG的生存率无差异。本研究表明,如果患者在HDCT/auto-SCT前能够达到CR或PR,儿童和青少年HGG患者HDCT/auto-SCT后的疗效令人鼓舞。