Chong Soon Eu, Mohamad Zaini Rhendra Hardy, Suraiya Siti, Lee Kok Tong, Lim Jo Anne
Department of Anaesthesiology and Intensive Care, School of Medical Sciences, Universiti Sains Malaysia, 16150, Kota Bharu, Kelantan, Malaysia.
Advanced Medical and Dental Institute, Universiti Sains Malaysia, Bertam, 13200, Kepala Batas, Penang, Malaysia.
Malar J. 2017 Jan 3;16(1):2. doi: 10.1186/s12936-016-1666-y.
Dengue and malaria are two common, mosquito-borne infections, which may lead to mortality if not managed properly. Concurrent infections of dengue and malaria are rare due to the different habitats of its vectors and activities of different carrier mosquitoes. The first case reported was in 2005. Since then, several concurrent infections have been reported between the dengue virus (DENV) and the malaria protozoans, Plasmodium falciparum and Plasmodium vivax. Symptoms of each infection may be masked by a simultaneous second infection, resulting in late treatment and severe complications. Plasmodium knowlesi is also a common cause of malaria in Malaysia with one of the highest rates of mortality. This report is one of the earliest in literature of concomitant infection between DENV and P. knowlesi in which a delay in diagnosis had placed a patient in a life-threatening situation.
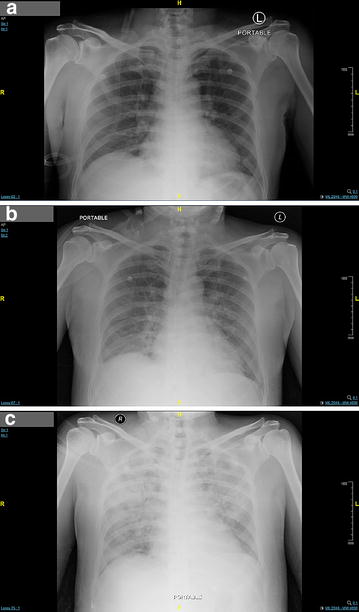
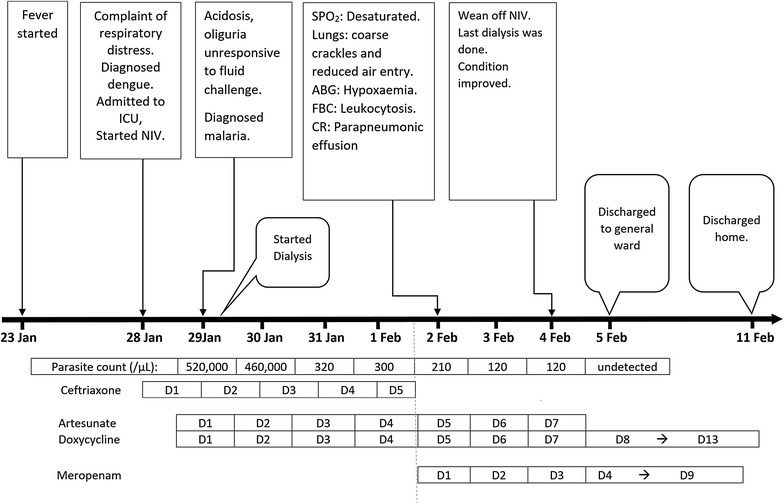
A 59-year old man staying near the Belum-Temengor rainforest at the Malaysia-Thailand border was admitted with fever for 6 days, with respiratory distress. His non-structural protein 1 antigen and Anti-DENV Immunoglobulin M tests were positive. He was treated for severe dengue with compensated shock. Treating the dengue had so distracted the clinicians that a blood film for the malaria parasite was not done. Despite aggressive supportive treatment in the intensive care unit (ICU), the patient had unresolved acidosis as well as multi-organ failure involving respiratory, renal, liver, and haematological systems. It was due to the presentation of shivering in the ICU, that a blood film was done on the second day that revealed the presence of P. knowlesi with a parasite count of 520,000/μL. The patient was subsequently treated with artesunate-doxycycline and made a good recovery after nine days in ICU.
This case contributes to the body of literature on co-infection between DENV and P. knowlesi and highlights the clinical consequences, which can be severe. Awareness should be raised among health-care workers on the possibility of dengue-malaria co-infection in this region. Further research is required to determine the real incidence and risk of co-infection in order to improve the management of acute febrile illness.
登革热和疟疾是两种常见的蚊媒感染疾病,若治疗不当可能导致死亡。由于其传播媒介的不同栖息地以及不同传播蚊子的活动,登革热和疟疾的合并感染较为罕见。首例报告病例发生于2005年。自那时起,已报告了数例登革热病毒(DENV)与疟原虫(恶性疟原虫和间日疟原虫)的合并感染病例。每种感染的症状可能会被同时发生的第二种感染所掩盖,从而导致治疗延迟和严重并发症。诺氏疟原虫也是马来西亚疟疾的常见病因之一,死亡率极高。本报告是文献中最早报道的DENV与诺氏疟原虫合并感染病例之一,其中诊断延迟使患者处于危及生命的境地。
一名59岁男子居住在马来西亚 - 泰国边境的勿洞 - 淡马鲁雨林附近,因发热6天伴呼吸窘迫入院。他的非结构蛋白1抗原和抗DENV免疫球蛋白M检测呈阳性。他因重度登革热伴代偿性休克接受治疗。对登革热的治疗使临床医生分心,以至于未进行疟原虫血涂片检查。尽管在重症监护病房(ICU)进行了积极的支持治疗,但患者的酸中毒仍未缓解,且出现了涉及呼吸、肾脏、肝脏和血液系统的多器官功能衰竭。由于患者在ICU出现寒战,在第二天进行了血涂片检查,结果显示存在诺氏疟原虫,寄生虫计数为520,000/μL。患者随后接受青蒿琥酯 - 多西环素治疗,在ICU住院九天后康复良好。
本病例丰富了关于DENV与诺氏疟原虫合并感染的文献资料,并突出了其可能产生的严重临床后果。应提高医护人员对该地区登革热 - 疟疾合并感染可能性的认识。需要进一步研究以确定合并感染的实际发病率和风险,从而改善急性发热性疾病的管理。