Department of General, Transplant and Liver Surgery, Medical University of Warsaw, Poland.
Department of Epidemiology, Medical University of Warsaw, Poland.
Sci Rep. 2017 Jan 6;7:39881. doi: 10.1038/srep39881.
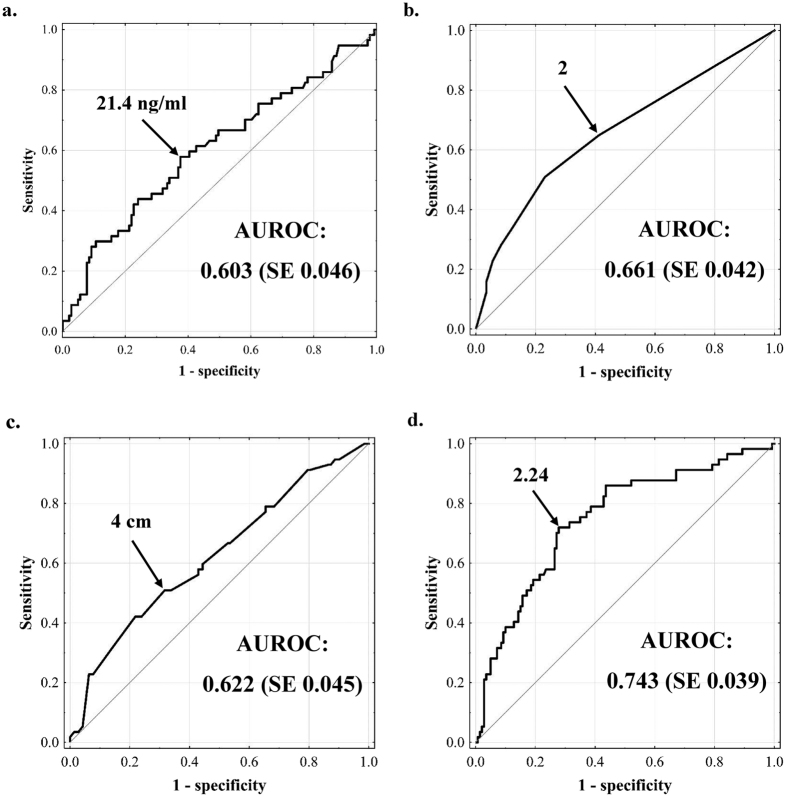
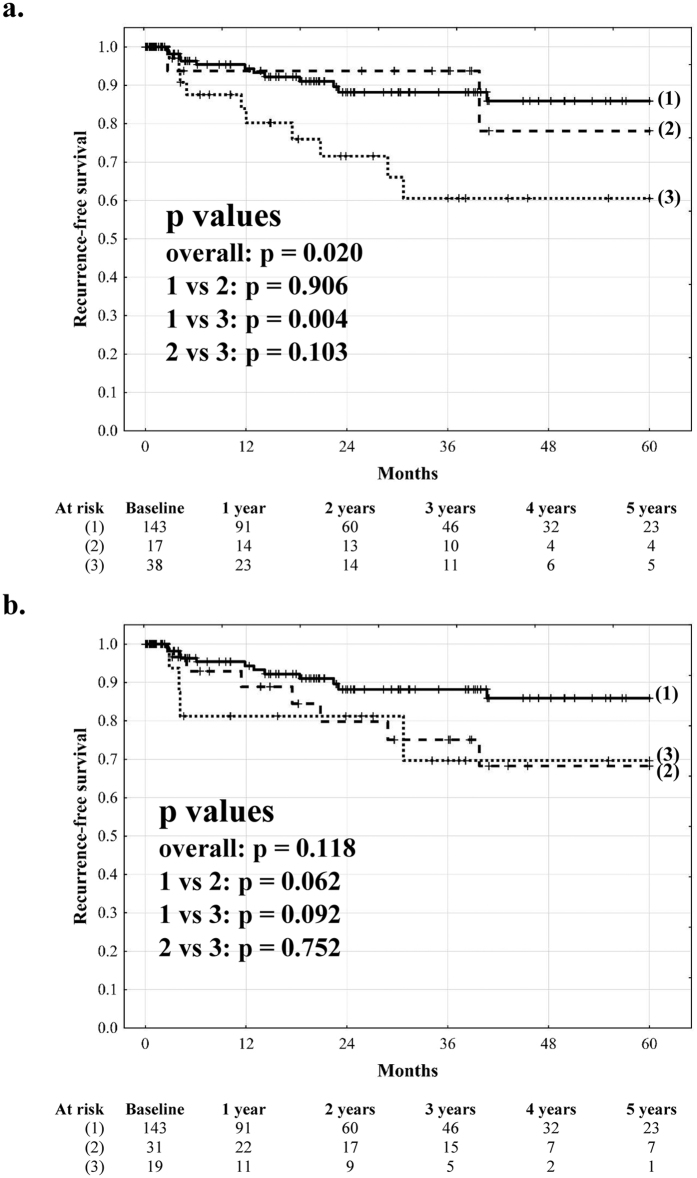
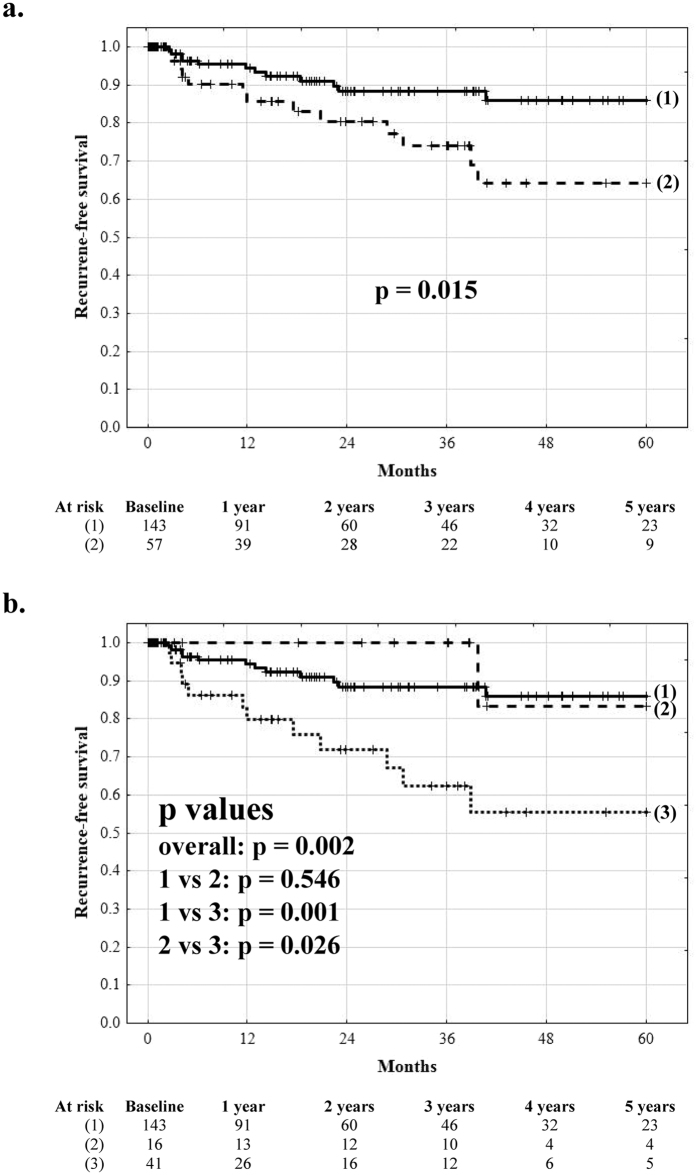
Microvascular invasion (MVI) is well known to negatively influence outcomes following surgical treatment of hepatocellular cancer (HCC) patients. The aim of this study was to evaluate the rationale for prediction of MVI before liver transplantation (LT). Data of 200 HCC patients after LT were subject to retrospective analysis. MVI was present in 57 patients (28.5%). Tumor number (p = 0.001) and size (p = 0.009), and alpha-fetoprotein (p = 0.049) were independent predictors of MVI used to create a prediction model, defined as: 0.293x(tumor number) + 0.283x(tumor size in cm) + 0.164xlog(alpha-fetoprotein in ng/ml) (c statistic = 0.743). The established cut-off (≥2.24) was associated with sensitivity and specificity of 72%. MVI was not an independent risk factor for recurrence (p = 0.307), in contrast to tumor number (p = 0.047) and size (p < 0.001), alpha-fetoprotein (p < 0.001) and poor differentiation (p = 0.039). Recurrence-free survival at 5 years for patients without MVI was 85.9% as compared to 83.3% (p = 0.546) and 55.3% (p = 0.001) for patients with false negative and true positive prediction of MVI, respectively. The use of both morphological and biological tumor features enables effective pre-transplant prediction of high-risk MVI. Provided that these parameters are combined in selection of HCC patients for LT, pre-transplant identification of all patients with MVI does not appear necessary.
微血管侵犯(MVI)已知会对接受肝细胞癌(HCC)手术治疗的患者的预后产生负面影响。本研究旨在评估在肝移植(LT)前预测 MVI 的合理性。对 200 例 LT 后 HCC 患者的数据进行回顾性分析。57 例患者(28.5%)存在 MVI。肿瘤数量(p=0.001)和大小(p=0.009)以及甲胎蛋白(p=0.049)是 MVI 的独立预测因子,用于创建预测模型,定义为:0.293x(肿瘤数量)+0.283x(肿瘤大小 cm)+0.164xlog(ng/ml 甲胎蛋白)(c 统计量=0.743)。确定的临界值(≥2.24)与 72%的敏感性和特异性相关。与肿瘤数量(p=0.047)、大小(p<0.001)、甲胎蛋白(p<0.001)和低分化(p=0.039)相比,MVI 不是复发的独立危险因素(p=0.307)。无 MVI 患者的 5 年无复发生存率为 85.9%,而 MVI 假阴性和真阳性预测的患者分别为 83.3%(p=0.546)和 55.3%(p=0.001)。使用形态学和生物学肿瘤特征可以有效预测 LT 前高危 MVI。只要这些参数结合起来用于选择 HCC 患者进行 LT,在 LT 前识别所有 MVI 患者似乎就没有必要。