Hepatic Surgery Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1095 Jiefang Avenue, Wuhan, 430030, China.
Translational Medicine Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, China.
BMC Cancer. 2020 Oct 31;20(1):1047. doi: 10.1186/s12885-020-07488-8.
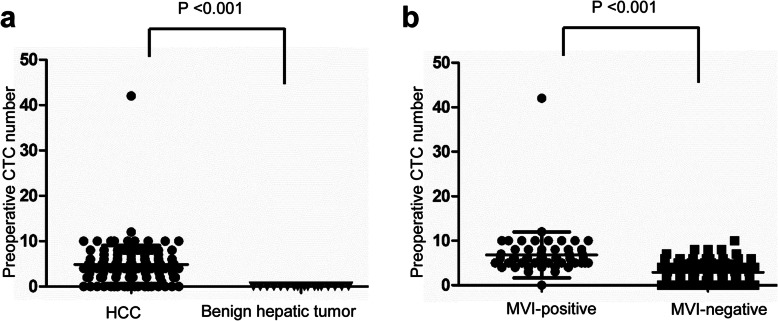
This study explored the diagnostic power of preoperative circulating tumor cells (CTCs) for the presence of microvascular invasion (MVI) and the relationship between dynamic changes in postoperative CTCs and prognosis.
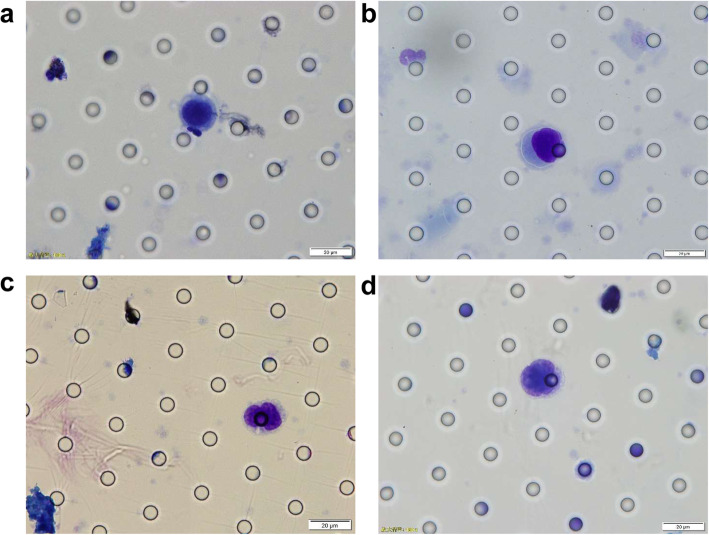
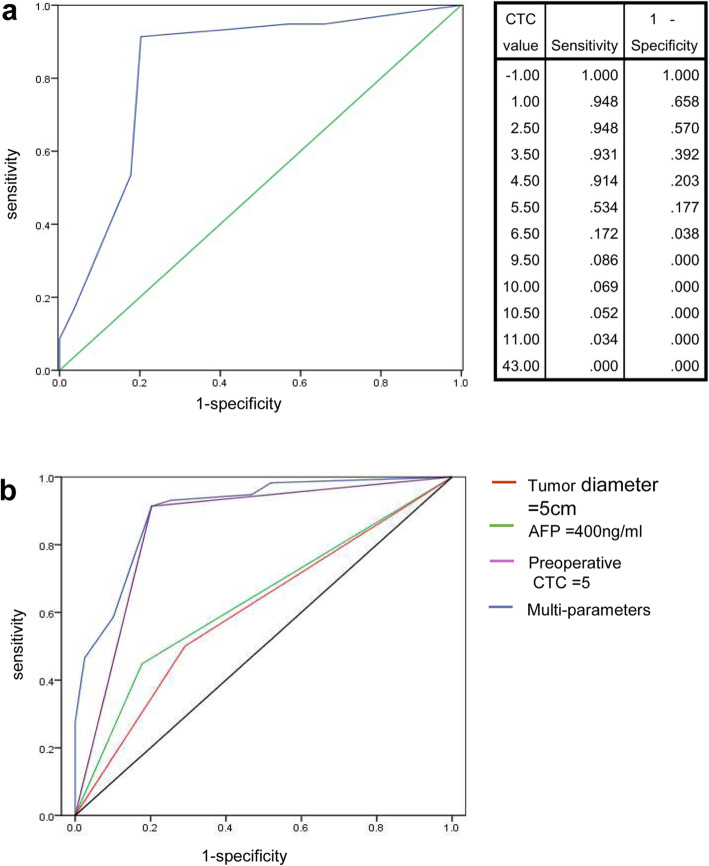
A total of 137 patients were recruited for the study. Preoperative blood samples were collected from all patients to detect CTCs. The time points for blood collection were before the operation, during the operation, and at 1 week, 1 month, 2 months, 3 months, 6 months, and 1 year after surgery. The predictive power of CTC count for the presence of MVI was analyzed by receiver operating characteristic (ROC) curve analysis. According to recurrence status, 137 patients were divided into three groups: no recurrence, early recurrence, and non-early recurrence groups.
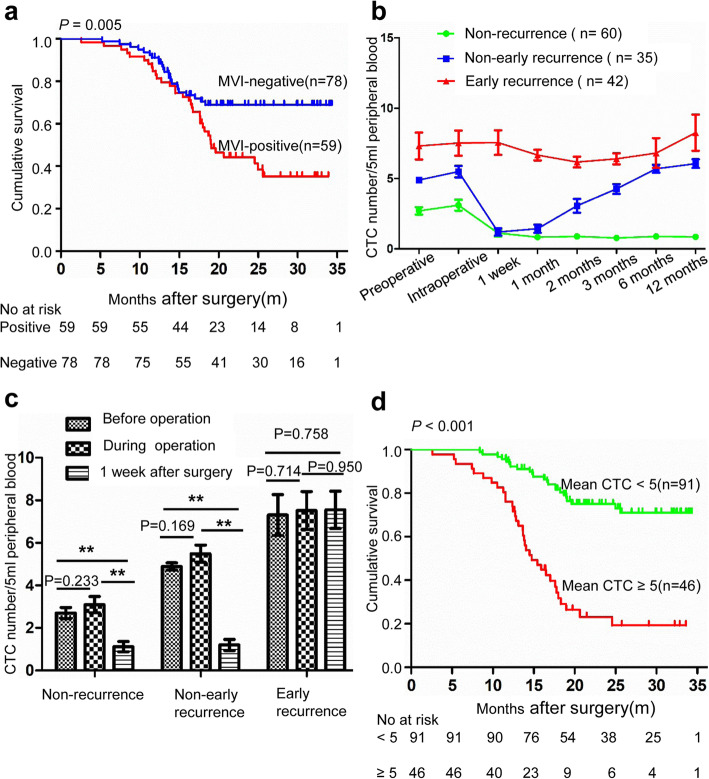
A threshold CTC count of 5 showed the most significant power for predicting the existence of MVI. In multivariate analysis, the parameters of preoperative CTC count, alpha-fetoprotein (AFP) and tumor diameter were independent predictors of MVI (P < 0.05). A CTC count greater than or equal to 5 had better predictive value than AFP > 400 μg/L and tumor diameter > 5 cm. The number of intraoperative CTCs in the three groups did not increase compared to that before surgery (P > 0.05). The number of CTCs in the nonrecurrence group and the non-early recurrence group decreased significantly 1 week after surgery compared with the intraoperative values (P < 0.001), although there was no significant difference in the early recurrence group (P = 0.95). Patients with mean CTC count ≥5 had significantly worse long-term outcomes than those with mean CTC count < 5 (P < 0.001).
The preoperative CTC counts in the peripheral blood of patients with HCC are closely correlated with MVI. The intraoperative manipulation of the lesion by the surgeon does not increase the number of CTCs in peripheral blood. Surgical removal of the tumor decreases the number of CTCs. The persistence of CTCs at a high level (≥ 5) after surgery suggests a risk of early recurrence.
Registration number is ChiCTR-OOC-16010183 , date of registration is 2016-12-18.
本研究旨在探讨术前循环肿瘤细胞(CTC)对微血管侵犯(MVI)存在的诊断能力,以及术后 CTC 动态变化与预后的关系。
共纳入 137 例患者进行研究。所有患者术前采集血样以检测 CTC。采血时间点为术前、术中及术后 1 周、1 个月、2 个月、3 个月、6 个月和 1 年。采用受试者工作特征(ROC)曲线分析 CTC 计数对 MVI 存在的预测能力。根据复发情况,137 例患者分为三组:无复发组、早期复发组和非早期复发组。
CTC 计数阈值为 5 时,预测 MVI 存在的能力最强。多因素分析显示,术前 CTC 计数、甲胎蛋白(AFP)和肿瘤直径是 MVI 的独立预测因素(P<0.05)。CTC 计数≥5 预测价值优于 AFP>400μg/L 和肿瘤直径>5cm。三组术中 CTC 数量与术前相比无明显增加(P>0.05)。与术中值相比,无复发组和非早期复发组术后 1 周 CTC 数量明显减少(P<0.001),但早期复发组无明显差异(P=0.95)。平均 CTC 计数≥5 的患者长期预后明显差于平均 CTC 计数<5 的患者(P<0.001)。
HCC 患者外周血中术前 CTC 计数与 MVI 密切相关。外科医生对病变的术中操作不会增加外周血中 CTC 的数量。肿瘤切除可减少 CTC 数量。术后 CTC 持续高水平(≥5)提示早期复发风险高。
注册号 ChiCTR-OOC-16010183,注册日期 2016-12-18。