Nath Anand, Yewale Sayali, Tran Tung, Brebbia John S, Shope Timothy R, Koch Timothy R
Anand Nath, Department of Medicine, MedStar-Washington Hospital Center and Georgetown University School of Medicine, Washington, DC 20010, United States.
World J Gastroenterol. 2016 Dec 21;22(47):10371-10379. doi: 10.3748/wjg.v22.i47.10371.
To evaluate the risks of medical conditions, evaluate gastric sleeve narrowing, and assess hydrostatic balloon dilatation to treat dysphagia after vertical sleeve gastrectomy (VSG).
VSG is being performed more frequently worldwide as a treatment for medically-complicated obesity, and dysphagia is common post-operatively. We hypothesize that post-operative dysphagia is related to underlying medical conditions or narrowing of the gastric sleeve. This is a retrospective, single institution study of consecutive patients who underwent sleeve gastrectomy from 2013 to 2015. Patients with previous bariatric procedures were excluded. Narrowing of a gastric sleeve includes: inability to pass a 9.6 mm gastroscope due to stenosis or sharp angulation or spiral hindering its passage.
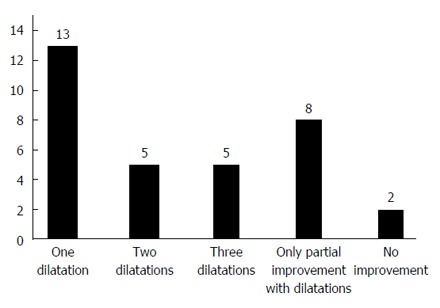
Of 400 consecutive patients, 352 are included; the prevalence of dysphagia is 22.7%; 33 patients (9.3%) have narrowing of the sleeve with 25 (7.1%) having sharp angulation or a spiral while 8 (2.3%) have a stenosis. All 33 patients underwent balloon dilatation of the gastric sleeve and dysphagia resolved in 13 patients (39%); 10 patients (30%) noted resolution of dysphagia after two additional dilatations. In a multivariate model, medical conditions associated with post-operative dysphagia include diabetes mellitus, symptoms of esophageal reflux, a low whole blood thiamine level, hypothyroidism, use of non-steroidal anti-inflammatory drugs, and use of opioids.
Narrowing of the gastric sleeve and gastric sleeve stenosis are common after VSG. Endoscopic balloon dilatations of the gastric sleeve resolves dysphagia in 69% of patients.
评估医疗状况风险,评估胃袖状切除术狭窄情况,并评估水囊扩张术治疗垂直袖状胃切除术(VSG)后吞咽困难的效果。
在全球范围内,VSG作为治疗伴有复杂医疗问题的肥胖症的方法,实施频率越来越高,且术后吞咽困难很常见。我们假设术后吞咽困难与潜在的医疗状况或胃袖状切除术狭窄有关。这是一项对2013年至2015年连续接受袖状胃切除术的患者进行的回顾性单机构研究。排除既往接受过减肥手术的患者。胃袖状切除术狭窄包括:因狭窄、锐角或螺旋状阻碍其通过而无法通过9.6毫米胃镜。
400例连续患者中,352例被纳入研究;吞咽困难的患病率为22.7%;33例患者(9.3%)存在胃袖状切除术狭窄,其中25例(7.1%)有锐角或螺旋状,8例(2.3%)有狭窄。所有33例患者均接受了胃袖状切除术的球囊扩张术,13例患者(39%)吞咽困难得到缓解;10例患者(30%)在额外进行两次扩张术后吞咽困难得到缓解。在多变量模型中,与术后吞咽困难相关的医疗状况包括糖尿病、食管反流症状、全血硫胺素水平低、甲状腺功能减退、使用非甾体抗炎药以及使用阿片类药物。
VSG术后胃袖状切除术狭窄和胃袖状切除术狭窄很常见。胃袖状切除术的内镜球囊扩张术使69%的患者吞咽困难得到缓解。