Heller Simon R, Bergenstal Richard M, White William B, Kupfer Stuart, Bakris George L, Cushman William C, Mehta Cyrus R, Nissen Steven E, Wilson Craig A, Zannad Faiez, Liu Yuyin, Gourlie Noah M, Cannon Christopher P
University of Sheffield, Sheffield, UK.
International Diabetes Center, Park-Nicollet Clinic, Minneapolis, Minnesota.
Diabetes Obes Metab. 2017 May;19(5):664-671. doi: 10.1111/dom.12871. Epub 2017 Feb 27.
To investigate relationships between glycated haemoglobin (HbA1c) and reported hypoglycaemia and risk of major adverse cardiovascular events (MACE).
The EXAMINE trial randomized 5380 patients with type 2 diabetes (T2DM) and a recent acute coronary syndrome (ACS) event, in 49 countries, to double-blind treatment with alogliptin or placebo in addition to standard of care. We used Cox proportional hazards models to analyse relationships among MACE, HbA1c levels and hypoglycaemic events.
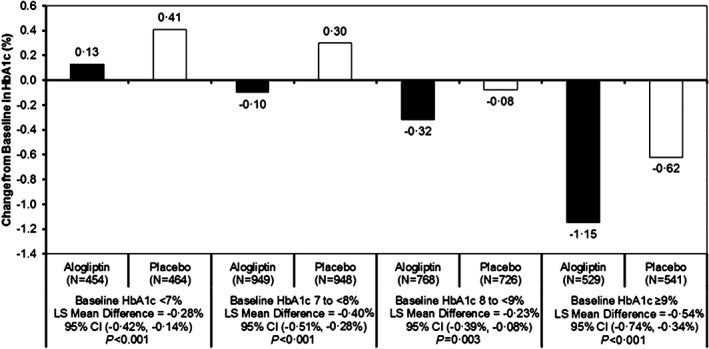
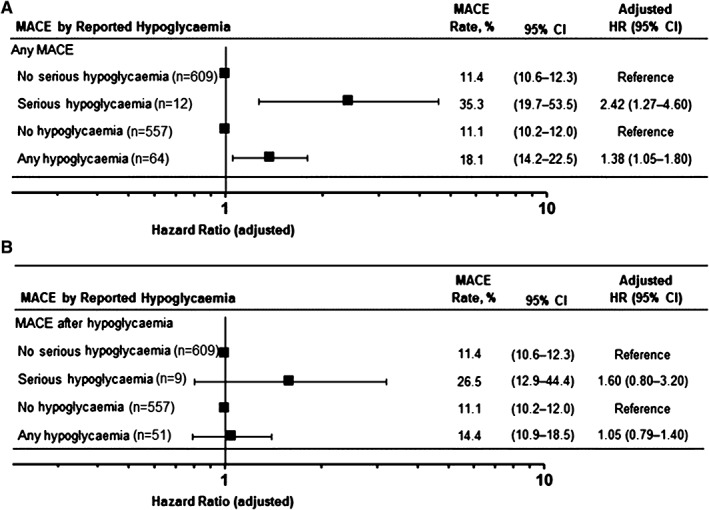
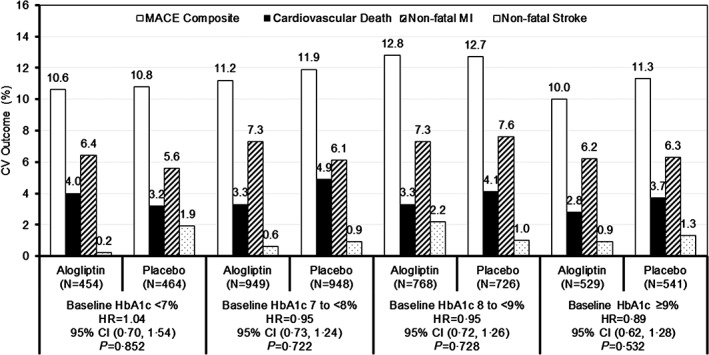
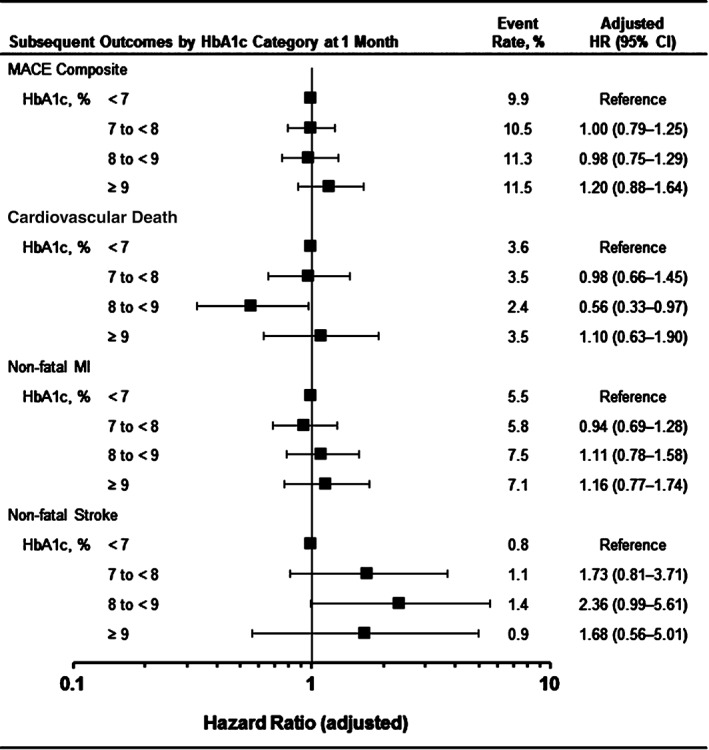
Patients randomized to alogliptin achieved lower HbA1c levels than the placebo group in all baseline HbA1c categories without differences in hypoglycaemia rates. No systematic change was found in MACE rates according to baseline HbA1c (P = 0.971) or HbA1c category at 1 month. Patients in the combined treatment groups (n = 5380) who experienced serious hypoglycaemia (n = 34) had higher MACE rates than those who did not (35.3% vs 11.4%, adjusted hazard ratio [HR] 2.42, 95% confidence interval [CI] 1.27-4.60; P = .007), although the association was less strong when analysing only events after the hypoglycaemic event (adjusted HR 1.60, 95% CI 0.80, 3.20).
There were no relationships between baseline HbA1c levels or HbA1c levels after 1 month of treatment and the risk of MACE. Alogliptin improved glycaemic control without increasing hypoglycaemia. Reported events of hypoglycaemia and serious hypoglycaemia were associated with MACE. These data underscore the safety of alogliptin in improving glycaemic control in T2DM post-ACS. Further study of hypoglycaemia as an independent risk factor for MACE in patients with T2DM and coronary disease is needed.
研究糖化血红蛋白(HbA1c)与报告的低血糖及主要不良心血管事件(MACE)风险之间的关系。
EXAMINE试验在49个国家将5380例2型糖尿病(T2DM)且近期发生急性冠脉综合征(ACS)事件的患者随机分为两组,在标准治疗基础上,分别接受阿格列汀或安慰剂双盲治疗。我们使用Cox比例风险模型分析MACE、HbA1c水平和低血糖事件之间的关系。
在所有基线HbA1c类别中,随机接受阿格列汀治疗的患者HbA1c水平低于安慰剂组,低血糖发生率无差异。根据基线HbA1c(P = 0.971)或治疗1个月时的HbA1c类别,MACE发生率未发现系统性变化。联合治疗组(n = 5380)中发生严重低血糖的患者(n = 34)的MACE发生率高于未发生严重低血糖的患者(35.3%对11.4%,调整后风险比[HR] 2.42,95%置信区间[CI] 1.27 - 4.60;P = 0.007),尽管仅分析低血糖事件后的事件时,这种关联强度较弱(调整后HR 1.60,95% CI 0.80,3.20)。
基线HbA1c水平或治疗1个月后的HbA1c水平与MACE风险之间无关联。阿格列汀改善血糖控制且不增加低血糖发生率。报告的低血糖和严重低血糖事件与MACE相关。这些数据强调了阿格列汀在改善ACS后T2DM患者血糖控制方面的安全性。需要进一步研究低血糖作为T2DM和冠心病患者MACE的独立危险因素。