Zhao Lin, Zhu Weiwei, Zhang Xiaojiang, He Dongfang, Guo Chengjun
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, 100029, Beijing, China.
BMC Cardiovasc Disord. 2017 Jan 6;17(1):16. doi: 10.1186/s12872-016-0445-6.
Whether diabetes mellitus (DM) is a predictor of long-term adverse clinical outcomes after repeat drug eluting stent (DES) implantation for DES in-stent restenosis (ISR) remains controversial. We sought to evaluate the effect of DM on the long-term clinical outcomes in patients undergoing repeat DES implantation for DES-ISR lesions.
In the present study, 254 patients with DES-ISR were divided into DM or non-DM groups according to the presence or absence of DM. All patients received repeat 2 generation DES implantation for DES-ISR. The occurrences of major adverse cardiac events (MACEs) over a 2-year follow-up period were compared between the two groups. MACEs were defined as cardiac death, myocardial infarction (MI), and target lesion revascularization (TLR). MACE free survival was investigated with Kaplan-Meier curve analysis. Cox regression analysis was used to identify factors associated with MACEs.
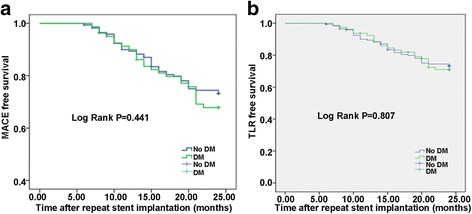
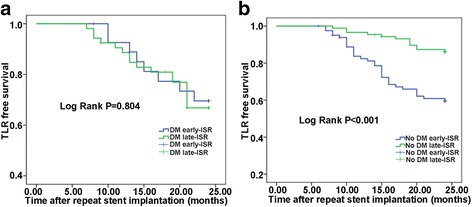
Baseline clinical characteristics were similar between groups, except for the prevalence of early restenosis (lower) in the DM group. Differences in angiographic and procedural characteristics were not significant between groups. The rates of 2-year MACE (30.9 vs. 26.0%; P = 0.453) and TLR (24.7 vs. 19.7%; P = 0.411) were similar between groups. MACE-free survival and TLR-free survival were also similar between groups (P = 0.441 and P = 0.807). Subgroup analysis suggested a significant difference in the MACE (39.0 vs.15.3%, P < 0.001) and TLR occurrence (30.5 vs.8.2%, P < 0.001) and TLR-free survival (lower in early subgroup, P < 0.001) between early and late occurrence of ISR in the non-DM group of patients but not in the DM group. After adjustment for all significant clinical variables, Cox regression analysis indicated that DM was not associated with MACEs (hazard ratio [HR] 1.531, 95% confidence interval [CI] 0.882-2.658, P =0.130). Non-focal type ISR and early ISR were predictors of MACEs (HR 2.671, 95% CI 1.468-4.858,P = 0.001; HR 4.703, 95% CI 2.725-8.117, P < 0.001, respectively).
Patients with DM have similar 2-year clinical outcomes to patients without DM when repeat 2 generation DES was used for treatment of DES-ISR. DM is not the predictor of long-term prognosis in patients undergoing repeat 2 generation DES for DES-ISR.
糖尿病(DM)是否为药物洗脱支架(DES)置入术后支架内再狭窄(ISR)患者长期不良临床结局的预测因素仍存在争议。我们旨在评估糖尿病对接受DES-ISR病变再次DES置入患者长期临床结局的影响。
在本研究中,254例DES-ISR患者根据是否患有糖尿病分为糖尿病组或非糖尿病组。所有患者均接受第二代DES再次置入以治疗DES-ISR。比较两组在2年随访期内主要不良心脏事件(MACE)的发生率。MACE定义为心源性死亡、心肌梗死(MI)和靶病变血运重建(TLR)。采用Kaplan-Meier曲线分析评估无MACE生存率。采用Cox回归分析确定与MACE相关的因素。
除糖尿病组早期再狭窄发生率较低外,两组基线临床特征相似。两组间血管造影和手术特征差异无统计学意义。两组间2年MACE发生率(30.9%对26.0%;P = 0.453)和TLR发生率(24.7%对19.7%;P = 0.411)相似。两组间无MACE生存率和无TLR生存率也相似(P = 0.441和P = 0.807)。亚组分析显示,非糖尿病组患者ISR早期和晚期发生时,MACE发生率(39.0%对15.3%,P < 0.001)、TLR发生率(30.5%对8.2%,P < 0.001)及无TLR生存率(早期亚组较低,P < 0.001)存在显著差异,而糖尿病组无此差异。在对所有显著临床变量进行校正后,Cox回归分析表明糖尿病与MACE无关(风险比[HR] 1.531,95%置信区间[CI] 0.882 - 2.658,P = 0.130)。非局灶性ISR和早期ISR是MACE的预测因素(HR 2.671,95% CI 1.468 - 4.858,P = 0.001;HR 4.703,95% CI 2.725 - 8.117,P < 0.001)。
当使用第二代DES治疗DES-ISR时,糖尿病患者与非糖尿病患者的2年临床结局相似。糖尿病并非接受第二代DES治疗DES-ISR患者长期预后的预测因素。