Docherty Mary, Shaw Kate, Goulding Lucy, Parke Hannah, Eassom Erica, Ali Farnoosh, Thornicroft Graham
South London and Maudsley NHS Foundation Trust, The Maudsley Hospital, Denmark Hill, London, SE5 8AF UK.
Centre for Implementation Science, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, UK.
Int J Ment Health Syst. 2017 Jan 5;11:8. doi: 10.1186/s13033-016-0115-1. eCollection 2017.
There is a significant treatment gap in provision of effective treatment for people with mental disorders globally. In some Low and Middle Income Countries (LMICs) this gap is 90% or more in terms of untreated cases. Clinical practice guidelines (CPGs) are one tool to improve health care provision. The aim of this review is to examine studies of the effectiveness of evidence-based CPG implementation across physical and mental health care, to inform mental healthcare provision in low and middle income countries (LMICs), and to identify transferable lessons from other non-communicable diseases to mental health.
A systematic literature review employing narrative synthesis and utilising the tools developed by the Cochrane Effective Practice and Organisation of Care (EPOC) group was conducted. Experimental studies of CPG implementation relating to non-communicable diseases, including mental disorders, in LMICs were retrieved and synthesised.
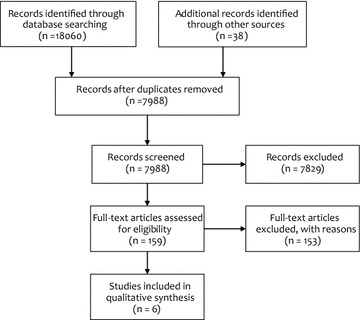
Few (six) studies were identified. Four cluster randomised controlled trials (RCTs) related to the introduction of CPGs for non-communicable diseases in physical health; one cluster-RCT included CPGs for both a non-communicable disease in physical health and mental health, and one uncontrolled before and after study described the introduction of a CPG for mental health. All of the included studies adopted multi-faceted CPG implementation strategies and used education as part of this strategy. Components of the multi-faceted strategies were sometimes poorly described. Results of the studies included generally show statistically significant improvement on some, but not all, outcomes.
Evidence for the effectiveness of interventions to improve uptake of, and compliance with, evidence-based CPGs in LMICs for mental disorders and for other non-communicable diseases is at present limited. The sparse literature does, however, suggest that multifaceted CPG implementation strategies that involve an educational component may be an effective way of improving guideline adherence and therefore of improving clinical outcomes. Further work is needed to examine cost-effectiveness of CPG implementation strategies in LMICs and to draw conclusions on the transferability of implementation experience in physical health care to mental health practice settings. Strategies to ensure that CPGs are developed with clear guidance for implementation, and with explicit, methods to evaluate them should be a priority for mental health researchers and for international agencies.
全球范围内,为精神障碍患者提供有效治疗方面存在显著的治疗差距。在一些低收入和中等收入国家(LMICs),就未治疗病例而言,这一差距达90%或更高。临床实践指南(CPGs)是改善医疗服务的一种工具。本综述的目的是审视基于证据的CPG在物理和精神卫生保健中实施效果的研究,为低收入和中等收入国家(LMICs)的精神卫生保健提供参考,并确定从其他非传染性疾病中可借鉴到精神卫生领域的经验教训。
采用叙述性综合法并利用Cochrane有效实践与护理组织(EPOC)小组开发的工具进行系统文献综述。检索并综合了关于低收入和中等收入国家(LMICs)中与包括精神障碍在内的非传染性疾病相关的CPG实施的实验性研究。
仅确定了六项研究。四项整群随机对照试验(RCTs)涉及在物理卫生保健中引入非传染性疾病的CPGs;一项整群RCT包括了物理卫生保健中的非传染性疾病和精神卫生的CPGs,一项非对照前后研究描述了精神卫生CPG的引入。所有纳入研究均采用多方面的CPG实施策略,并将教育作为该策略的一部分。多方面策略的组成部分有时描述不佳。纳入研究的结果总体显示,在部分而非所有结局上有统计学显著改善。
目前,关于在低收入和中等收入国家(LMICs)改善基于证据的CPGs在精神障碍及其他非传染性疾病中的采用率和依从性的干预措施有效性的证据有限。然而,稀少的文献确实表明,涉及教育成分的多方面CPG实施策略可能是提高指南依从性从而改善临床结局的有效方法。需要进一步开展工作,以审视低收入和中等收入国家(LMICs)中CPG实施策略的成本效益,并就物理卫生保健中的实施经验向精神卫生实践环境的可转移性得出结论。确保CPGs在制定时具有明确的实施指南以及明确的评估方法,应是精神卫生研究人员和国际机构的优先事项。