Schaefer Tim, Satzger Imke, Gutzmer Ralf
Department for Dermatology and Allergy, Skin Cancer Center Hannover (HTZH), Hannover Medical School Office for Dermatology, Allergy and Venerology, Seelze, Germany.
Medicine (Baltimore). 2017 Jan;96(1):e5753. doi: 10.1097/MD.0000000000005753.
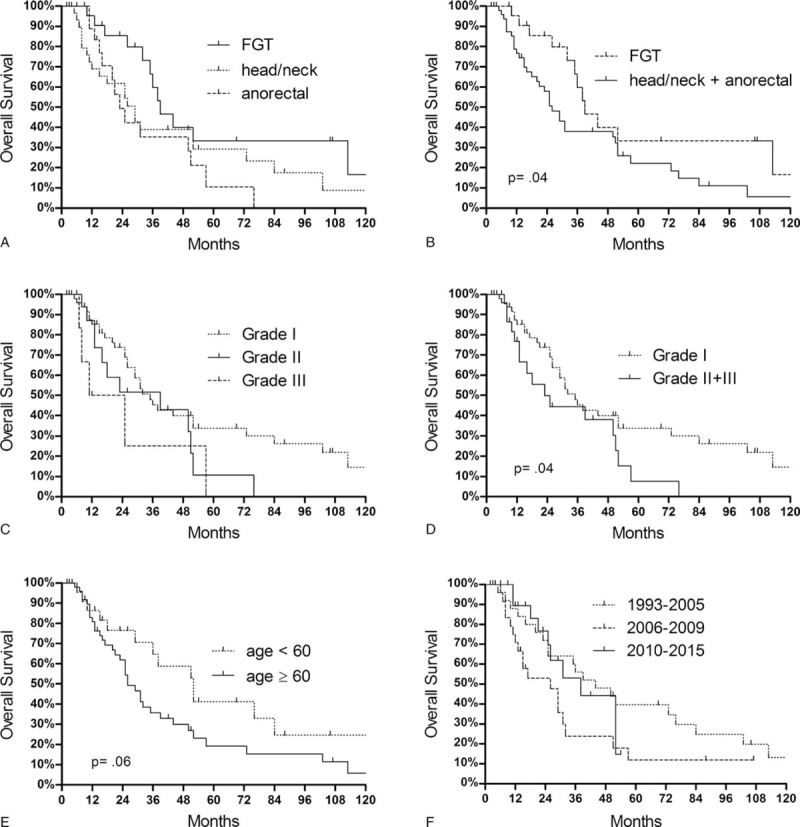
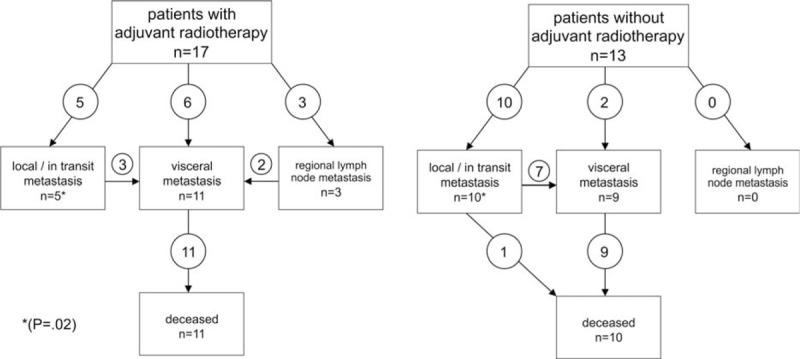
Mucosal melanomas represent a rare entity with different risk factors and molecular features compared to cutaneous melanomas. They arise most commonly from mucosal surfaces in the head/neck region, the female genital tract (FGT) and the anorectal region. The aim of this study was to evaluate clinics, prognosis, and treatment options of patients with mucosal melanoma, in particular with regard to different primary sites.We retrospectively analyzed 75 patients with mucosal melanomas diagnosed in the years 1993 to 2015 in our department. The primary melanomas were located in the head/neck region (n = 32), the FGT (n = 24), and the anorectal region (n = 19).The median age of the patients was 66 years. At initial diagnosis the primary melanoma was not completely resectable in 11 (15%) patients, 18 (24%) patients had regional lymph node metastases, and 7 (9%) patients distant metastases. During follow-up, 22 (29%) patients suffered from a local recurrence, in particular patients with primary melanoma in the head/neck region without postoperative radiotherapy. By multivariate analysis location of the primary melanoma in the head/neck area or anorectal region and presence of metastases at time of diagnosis represented poor prognostic factors for recurrence-free survival. In 62 tested individuals 7 KIT mutations were found, 2 BRAF mutations in 57 tested patients. Four patients received targeted therapies, 14 checkpoint inhibitors, 4 (1/1 on vemurafenib, 1/7 on ipilimumab, and 2/7 on PD-1 inhibitors) patients showed responses of more than 100 days duration.Mucosal melanomas are often locally advanced or metastatic at initial diagnosis, thus they require extensive staging procedures. The high rate of local recurrences in the head/neck region can be significantly reduced by postoperative radiotherapy. For the potential use of medical treatment a mutation analysis for KIT and BRAF genes should be performed. The use of new immunologic and targeted therapies has to be further evaluated.
黏膜黑色素瘤是一种罕见的疾病,与皮肤黑色素瘤相比,具有不同的危险因素和分子特征。它们最常见于头颈部区域、女性生殖道(FGT)和肛管直肠区域的黏膜表面。本研究的目的是评估黏膜黑色素瘤患者的临床情况、预后和治疗选择,特别是针对不同的原发部位。我们回顾性分析了1993年至2015年在我们科室诊断的75例黏膜黑色素瘤患者。原发性黑色素瘤位于头颈部区域(n = 32)、FGT(n = 24)和肛管直肠区域(n = 19)。患者的中位年龄为66岁。在初次诊断时,11例(15%)患者的原发性黑色素瘤无法完全切除,18例(24%)患者有区域淋巴结转移,7例(9%)患者有远处转移。在随访期间,22例(29%)患者出现局部复发,特别是头颈部区域原发性黑色素瘤且未接受术后放疗的患者。多因素分析显示,原发性黑色素瘤位于头颈部区域或肛管直肠区域以及诊断时存在转移是无复发生存的不良预后因素。在62例检测个体中发现了7个KIT突变,在57例检测患者中发现了2个BRAF突变。4例患者接受了靶向治疗,14例接受了检查点抑制剂治疗,4例(1/1接受维莫非尼治疗,1/7接受伊匹木单抗治疗,2/7接受PD - 1抑制剂治疗)患者显示出持续时间超过100天的反应。黏膜黑色素瘤在初次诊断时通常处于局部晚期或已转移,因此需要进行广泛的分期检查。术后放疗可显著降低头颈部区域的局部复发率。对于药物治疗的潜在应用,应进行KIT和BRAF基因的突变分析。新的免疫治疗和靶向治疗的应用必须进一步评估。