Heldal Kristian, Hartmann Anders, Lønning Kjersti, Leivestad Torbjørn, Reisæter Anna V, Line Pål-Dag, Holdaas Hallvard, Midtvedt Karsten
Department of Cardiology, Nephrology, Endocrinology and Geriatrics, Clinic of Internal Medicine, Telemark Hospital Trust, N-3710, Skien, Norway.
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
BMC Nephrol. 2017 Jan 11;18(1):13. doi: 10.1186/s12882-016-0426-0.
Age and number of recipients in need of kidney re-transplantation are increasing. Re-transplantation practices and outcomes in elderly recipients are not previously explored. We aimed to retrospectively evaluate the outcomes of recipients 65 years and older receiving their second deceased donor allograft.
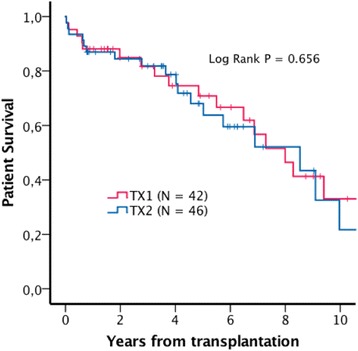
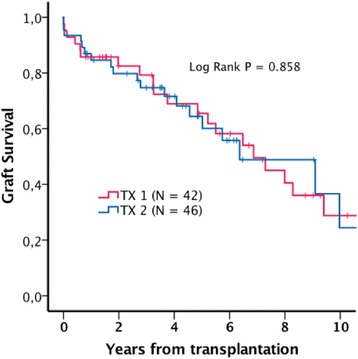
The study was designed as a retrospective registry based study. All recipients 65 years or older who received a deceased donor kidney transplant at Oslo University Hospital between 2000 and 2014 were included in the study. Survival outcomes were compared between recipients of first (TX1) and second (TX2) allograft. Survival analyses were performed using the Kaplan-Meier method and Cox proportional hazard models with patient survival, uncensored graft survival and death-censored graft survival as outcomes in the analyses.
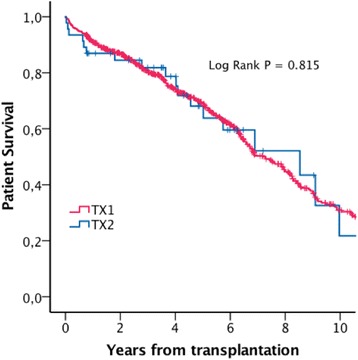
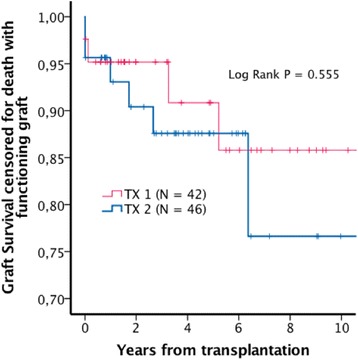
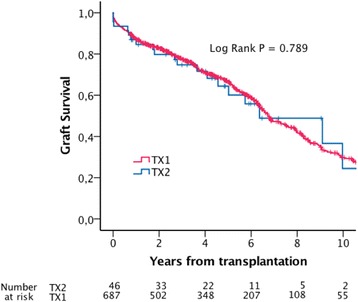
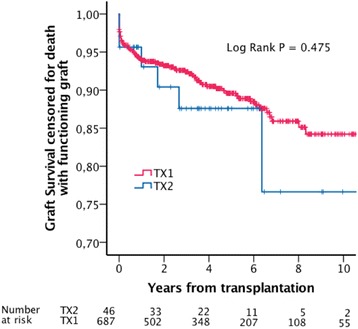
Seven hundred and thirty-tree recipients > 65 years received a first (n = 687) or second (n = 46) deceased donor kidney transplant. Five years uncensored graft survival rates were 64% in TX 2 and 67% in TX 1 (P= 0.789). Estimated five years graft survival rates censored for death with functioning graft were 88% in TX2 and 90% in TX1 (P=0.475). Adjusted hazard ratio for uncensored graft loss (TX2 vs. TX1) was 1.24 (95% CI 0.77 - 2.00). Adjusted hazard ratio for graft loss censored for death with functioning graft (TX2 vs. TX1) was 1.70 (0.72-4.02).
Older recipients of second transplants have outcomes that are comparable to the outcomes of age-matched first transplant recipients, and far better than previously documented for older transplant candidates remaining on dialysis treatment. Advanced age by itself should not be a contraindication for re-transplantation. Best results are achieved with short time on dialysis before re-transplantation.
需要再次肾移植的受者年龄和数量正在增加。老年受者的再次移植实践和结果此前尚未得到探讨。我们旨在回顾性评估65岁及以上接受第二次尸体供肾移植的受者的结局。
本研究设计为一项基于回顾性登记的研究。纳入2000年至2014年期间在奥斯陆大学医院接受尸体供肾移植的所有65岁及以上受者。比较首次(TX1)和第二次(TX2)移植受者的生存结局。采用Kaplan-Meier法和Cox比例风险模型进行生存分析,分析中的结局包括患者生存、未删失移植物生存和死亡删失移植物生存。
733名65岁以上受者接受了首次(n = 687)或第二次(n = 46)尸体供肾移植。TX2组5年未删失移植物生存率为64%,TX1组为67%(P = 0.789)。对于有功能移植物的死亡删失的5年移植物生存率估计,TX2组为88%,TX1组为90%(P = 0.475)。未删失移植物丢失的调整风险比(TX2与TX1)为1.24(95%CI 0.77 - 2.00)。对于有功能移植物的死亡删失的移植物丢失的调整风险比(TX2与TX1)为1.70(0.72 - 4.02)。
第二次移植的老年受者的结局与年龄匹配的首次移植受者的结局相当,并且远优于之前记录的仍接受透析治疗的老年移植候选者的结局。高龄本身不应成为再次移植的禁忌证。再次移植前透析时间短可取得最佳效果。