Gao Zhidong, Wang Chao, Xue Qian, Wang Jingtong, Shen Zhanlong, Jiang Kewei, Shen Kai, Liang Bin, Yang Xiaodong, Xie Qiwei, Wang Shan, Ye Yingjiang
Department of Gastrointestinal Surgery, Peking University People's Hospital, Beijing, 100044, People's Republic of China.
Department of Gastroenterology and Endoscopy, Peking University People's Hospital, Beijing, 100044, People's Republic of China.
BMC Gastroenterol. 2017 Jan 11;17(1):8. doi: 10.1186/s12876-016-0567-4.
The detectable rate of minimal gastric GISTs has continuously increased. While the surveillance and management of GIST <2 cm have been deemed controversial or lack evidence-based approaches. The aim of the current study is to propose a cut-off value of tumor size for treatment policy and the appropriate timing for endoscopic ultrasonography (EUS) follow-up in the minimal EUS-suspected gastric GIST patients.
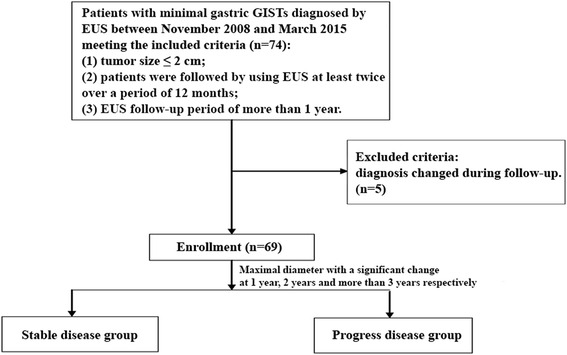
A single-institution retrospective study was performed. 69 patients with EUS-suspected gastric GISTs were studied from November 2008 to March 2015. 69 patients with minimal gastric GISTs ≤2 cm diagnosed by EUS were followed for a mean period of 29 months (range, 12 to 70). An at least 20% increase of the maximal diameter of the tumors was set as a significant change.
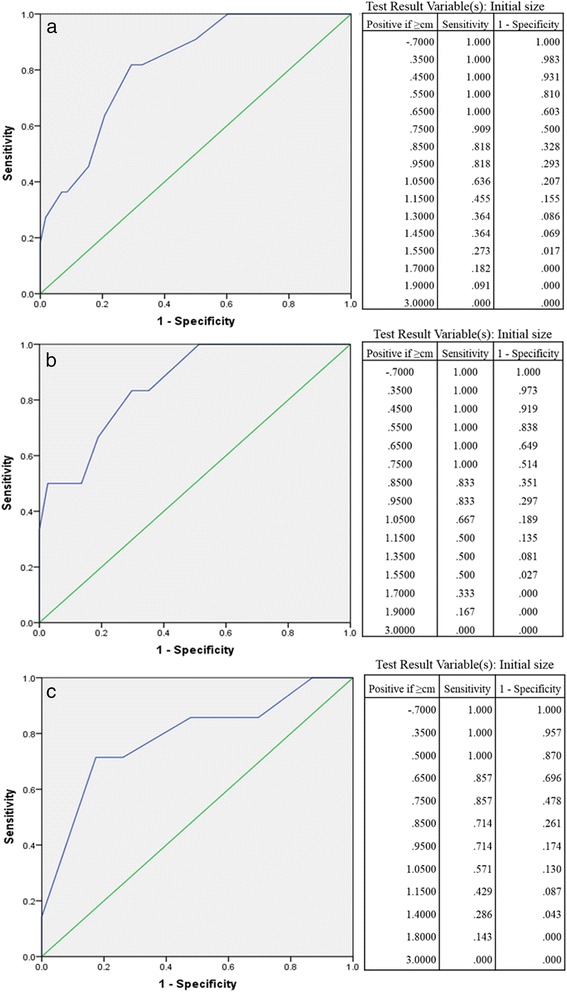
During follow-up, Of the 69 minimal EUS-suspected GISTs, 16 (23.2%) showed significant changes in size. 11 out of 69 GISTs (15.9%), 6 out of 43 GISTs (14.0%), 7 out of 30 GISTs (23.3%) showed significant changes in size, at 1 year, 2 years, and more than 3 years respectively. The receiver operating characteristic curve analysis showed that the tumor size cut-off was 9.5 mm. Only 4.7 and 3.7% of gastric EUS-suspected GISTs of <9.5 mm in size showed significant changes at 1 year and 2 years, while 9.5% at more than 3 years. 34.6, 31.3 and 55.6% of gastric EUS-suspected GISTs of ≥ 9.5 mm in size showed significant changes at 1 year, 2 years and more than 3 years.
Minimal EUS-suspected GISTs, larger than 9.5 mm may be associated with significant progression. The patients with a ≥ 9.5 mm GIST should have a EUS 6-12months, while <9.5 mm GIST may have a EUS extended to every 2-3 years.
微小胃间质瘤的检出率持续上升。而对于直径<2 cm的间质瘤的监测和管理一直存在争议或缺乏循证方法。本研究的目的是提出针对治疗策略的肿瘤大小截断值,以及针对内镜超声(EUS)怀疑为微小胃间质瘤患者进行EUS随访的合适时机。
进行单中心回顾性研究。对2008年11月至2015年3月期间69例EUS怀疑为胃间质瘤的患者进行研究。对69例经EUS诊断为直径≤2 cm的微小胃间质瘤患者进行了平均29个月(范围12至70个月)的随访。将肿瘤最大直径至少增加20%设定为有显著变化。
随访期间,69例EUS怀疑为微小间质瘤的患者中,16例(23.2%)肿瘤大小有显著变化。69例间质瘤中11例(15.9%)、43例间质瘤中6例(14.0%)、30例间质瘤中7例(23.3%)分别在1年、2年和3年以上出现肿瘤大小显著变化。受试者工作特征曲线分析显示肿瘤大小截断值为9.5 mm。直径<9.5 mm的EUS怀疑为胃间质瘤的患者中,仅4.7%和3.7%在1年和2年时出现显著变化,而在3年以上时为9.5%。直径≥9.5 mm的EUS怀疑为胃间质瘤的患者中,34.6%、31.3%和55.6%分别在1年、2年和3年以上出现显著变化。
EUS怀疑为微小的、直径大于9.5 mm的间质瘤可能与显著进展相关。直径≥9.5 mm的间质瘤患者应每6 - 12个月进行一次EUS检查,而直径<9.5 mm的间质瘤患者EUS检查间隔可延长至每2 - 3年一次。