Koçyiğit Cemil, Çatlı Gönül, İnce Gülberat, Özkan Elif Büşra, Dündar Bumin Nuri
İzmir Katip Çelebi University Faculty of Medicine, Department of Pediatric Endocrinology, İzmir, Turkey, E-mail:
J Clin Res Pediatr Endocrinol. 2017 Jun 1;9(2):150-155. doi: 10.4274/jcrpe.3842. Epub 2017 Jan 12.
Stoss vitamin D treatment has been recommended for its non-skeletal benefits in adults, but there is a lack of data on the optimal dose of vitamin D stoss therapy in children with vitamin D deficiency/insufficiency without rickets. This study aimed to compare efficiency/side effects of two different stoss therapy regimens (10 000 IU/kg and 300 000 IU vitamin D3) administered in children with vitamin D deficiency/insufficiency without rickets.
Sixty-four children who had vitamin D deficiency/insufficiency were studied. A serum 25-hydroxyvitamin-D (25-OH-D) level of 15-20 ng/mL was considered as vitamin D insufficient and <15 ng/mL was considered as vitamin D deficient. The patients were divided into two groups according to the stoss therapy doses they received. Serum calcium, phosphate, alkaline phosphatase, 25-OH-D, parathyroid hormone levels, and spot urine calcium/creatinine ratios before/after treatment were recorded. Wrist radiography and renal ultrasonography were performed.
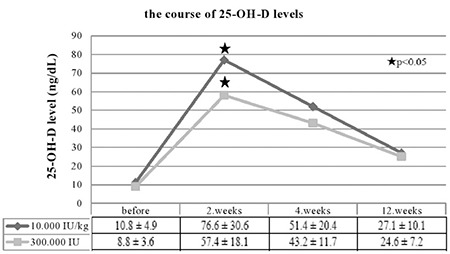
The mean age of the subjects was 10.6±4.4 years. Thirty-two children were treated with a single vitamin D3 dose of 10 000 IU/kg and 32 patients received 300 000 IU. No difference was found in 25-OH-D levels between the two groups at presentation. The mean level of 25-OH-D was higher in the 10 000 IU/kg group at the second week of therapy. There was no difference between the groups at post-treatment weeks 4 and 12. The 25-OH-D was found to be below optimal levels (≥30 ng/mL) in 66.5% and <20 ng/mL in 21.8% of patients at the third month in both groups. None developed hypercalcemia and/or hypercalciuria. Nephrolithiasis was not detected in any patient.
This study showed that both doses of stoss therapy used in the treatment of vitamin D insufficiency/deficiency are effective and safe. However, an optimal level of 25-OH-D cannot be maintained for more than three months.
冲击性维生素D治疗因其对成人的非骨骼益处而被推荐,但对于无佝偻病的维生素D缺乏/不足儿童,缺乏关于维生素D冲击治疗最佳剂量的数据。本研究旨在比较两种不同冲击治疗方案(10000IU/kg和30万IU维生素D3)在无佝偻病的维生素D缺乏/不足儿童中的疗效/副作用。
对64名维生素D缺乏/不足的儿童进行研究。血清25-羟维生素D(25-OH-D)水平为15-20ng/mL被视为维生素D不足,<15ng/mL被视为维生素D缺乏。根据患者接受的冲击治疗剂量将其分为两组。记录治疗前后的血清钙、磷、碱性磷酸酶、25-OH-D、甲状旁腺激素水平以及随机尿钙/肌酐比值。进行腕部X线摄影和肾脏超声检查。
受试者的平均年龄为10.6±4.4岁。32名儿童接受单次10000IU/kg的维生素D3剂量治疗,32名患者接受30万IU治疗。两组治疗前25-OH-D水平无差异。治疗第二周时,10000IU/kg组的25-OH-D平均水平较高。治疗后第4周和第12周两组之间无差异。两组在第三个月时,66.5%的患者25-OH-D低于最佳水平(≥30ng/mL),21.8%的患者<20ng/mL。无一例发生高钙血症和/或高钙尿症。未在任何患者中检测到肾结石。
本研究表明,用于治疗维生素D不足/缺乏的两种冲击治疗剂量均有效且安全。然而,25-OH-D的最佳水平无法维持超过三个月。