Yang Shih-Cheng, Hsu Chien-Ning, Liang Chih-Ming, Tai Wei-Chen, Wu Cheng-Kun, Shih Chih-Wei, Ku Ming-Kun, Yuan Lan-Ting, Wang Jiunn-Wei, Tseng Kuo-Lun, Hung Tsung-Hsing, Nguang Seng-Howe, Hsu Pin-I, Wu Deng-Chyang, Chuah Seng-Kee
Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan.
Department of Pharmacy, Kaohsiung Gang Gung Memorial Hospital, Kaohsiung, Taiwan; School of Pharmacy, Kaohsiung Medical University, Kaohsiung, Taiwan.
PLoS One. 2017 Jan 12;12(1):e0168918. doi: 10.1371/journal.pone.0168918. eCollection 2017.
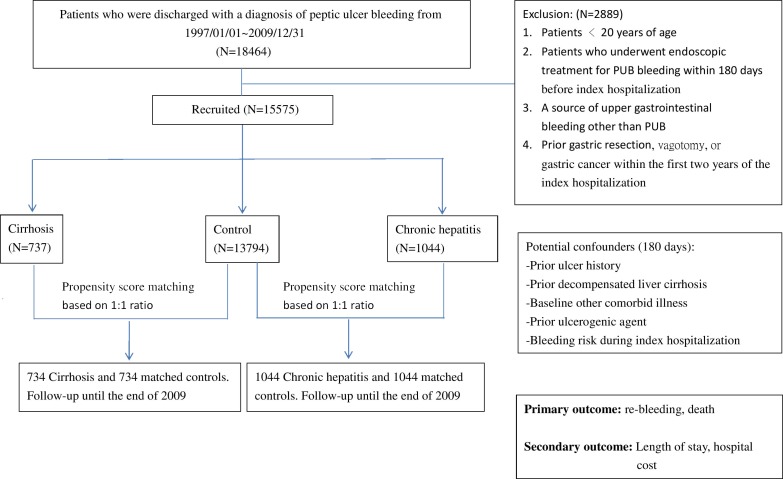
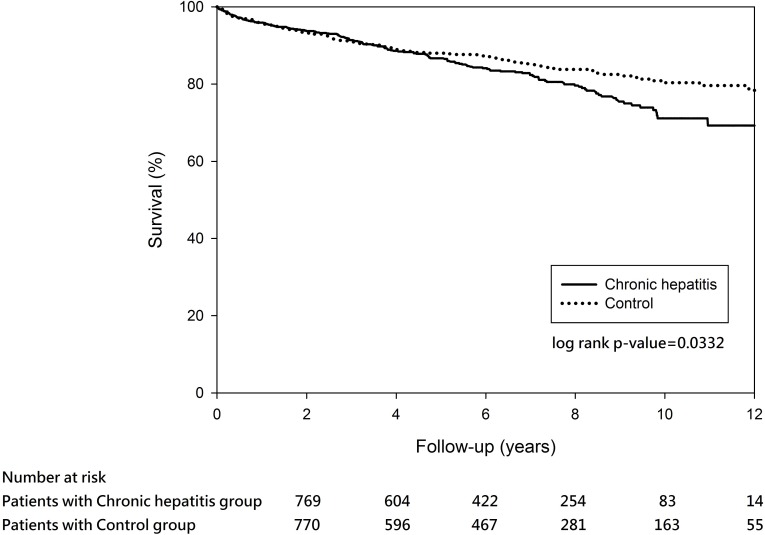
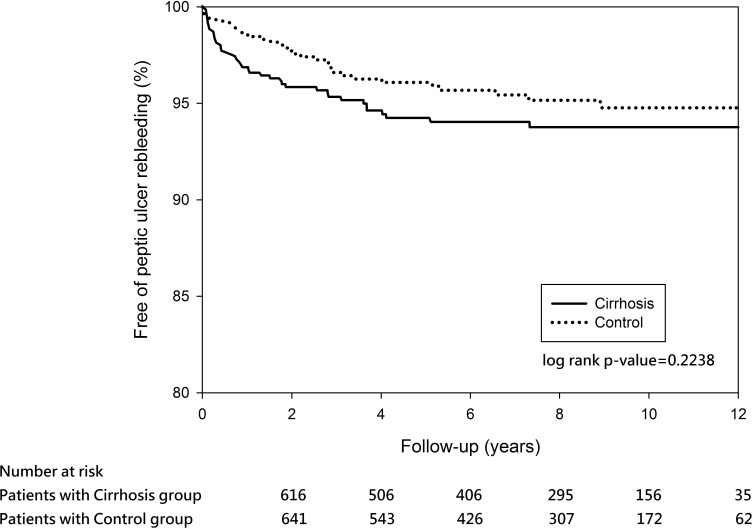
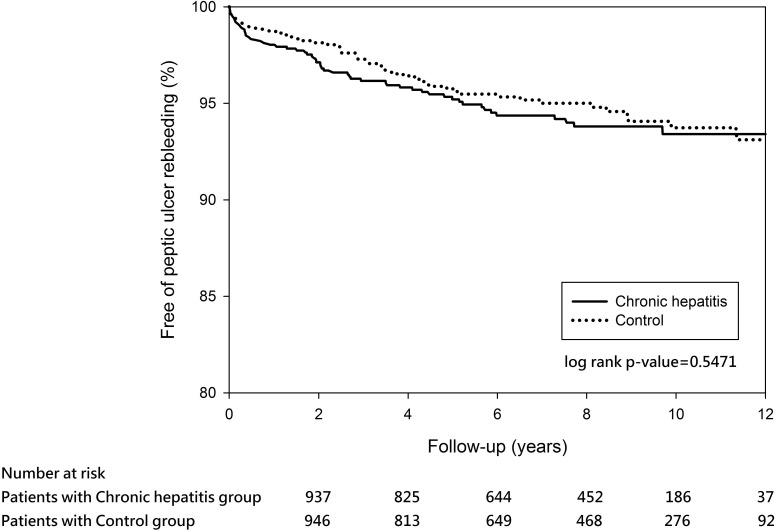
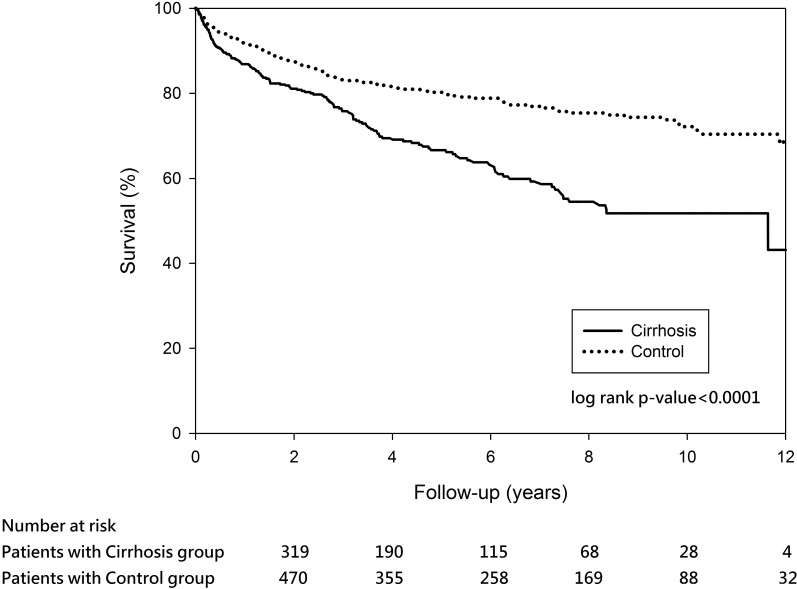
Although a few studies have investigated the risks of peptic ulcer bleeding (PUB) in cirrhotic patients, large population-based studies on in-hospital and long-term reports on recurrent PUB in a cohort of cirrhotic patients are lacking. This 12-year nationwide cohort study aimed to investigate the risks of in-hospital and long-term rebleeding and mortality in cirrhotic patients and to identify possible risk factors. Patient data from 1997 to 2008 were extracted from the National Health Insurance Research Database in Taiwan. A total of 15,575 patients who were discharged with a diagnosis of PUB were identified after strict exclusions (n = 2889). Among them, patients with cirrhosis (n = 737) and those with chronic hepatitis (n = 1044) were compared to propensity-score matched normal controls at a ratio of 1:1. Accumulated in-hospital and long-term follow-up PUB-free survival rates were analyzed in patients with cirrhosis, patients with chronic hepatitis, and matched controls. Cox proportional hazards regression was used to identify each independent risk factor. Compared with matched controls, patients with cirrhosis exhibited a 2.62-fold (95% CI: 1.74-3.92) higher risk of developing in-hospital rebleeding, but the risk of long-term rebleeding was comparable between cirrhotic patients and matched controls (hazard ratio: 1.29, 95% CI: 0.8-2.09). On the other hand, no significant difference was observed in in-hospital and long-term rebleeding between chronic hepatitis patients and matched controls. We compared the survival rates of cirrhotic and chronic hepatitis patients to that of matched controls. After propensity score matching, both cirrhotic and chronic hepatitis patients showed significantly lower survival than the matched controls (P < 0.0001 and 0.033, respectively) during the 12-year follow-up period. However, in-hospital and long-term rebleeding rates were not significantly different between chronic hepatitis patients and matched controls (P = 0.251 and 0.474, respectively). In conclusion, liver cirrhosis increased health care expenses in patients with PUB and these patients exhibited higher recurrent bleeding rate than non-cirrhotic patients during hospitalization. Cirrhosis and chronic hepatitis are independently associated with an increased long-term mortality when compared with patients without liver disease.
尽管有一些研究调查了肝硬化患者消化性溃疡出血(PUB)的风险,但缺乏基于大样本人群的肝硬化患者住院期间及复发性PUB长期报告的研究。这项为期12年的全国性队列研究旨在调查肝硬化患者住院期间及长期再出血和死亡的风险,并确定可能的危险因素。从台湾国民健康保险研究数据库中提取了1997年至2008年的患者数据。经过严格排除(n = 2889)后,共确定了15575例诊断为PUB出院的患者。其中,将肝硬化患者(n = 737)和慢性肝炎患者(n = 1044)与倾向评分匹配的正常对照按1:1的比例进行比较。分析了肝硬化患者、慢性肝炎患者和匹配对照的累积住院期间及长期随访无PUB生存率。采用Cox比例风险回归分析确定各独立危险因素。与匹配对照相比,肝硬化患者发生住院再出血的风险高2.62倍(95%CI:1.74 - 3.92),但肝硬化患者与匹配对照的长期再出血风险相当(风险比:1.29,95%CI:0.8 - 2.09)。另一方面,慢性肝炎患者与匹配对照在住院期间及长期再出血方面未观察到显著差异。我们比较了肝硬化和慢性肝炎患者与匹配对照的生存率。倾向评分匹配后,在12年随访期间,肝硬化和慢性肝炎患者的生存率均显著低于匹配对照(分别为P < 0.0001和0.033)。然而,慢性肝炎患者与匹配对照的住院期间及长期再出血率无显著差异(分别为P = 0.251和0.474)。总之,肝硬化增加了PUB患者的医疗费用,这些患者在住院期间的再出血复发率高于非肝硬化患者。与无肝病患者相比,肝硬化和慢性肝炎独立地与长期死亡率增加相关。