Gargiulo Giuseppe, Stabile Eugenio, Ferrone Marco, Barbato Emanuele, Zimmermann Frederik M, Adjedj Julien, Hennigan Barry, Matsumura Mitsuaki, Johnson Nils P, Fearon William F, Jeremias Allen, Trimarco Bruno, Esposito Giovanni
Department of Advanced Biomedical Sciences, University of Naples Frederico II, Naples, Italy.
Cardiovascular Center, OLV Clinic, Aalst, Belgium.
Cardiovasc Diabetol. 2017 Jan 13;16(1):7. doi: 10.1186/s12933-016-0494-2.
Adenosine-free coronary pressure wire metrics have been proposed to test the functional significance of coronary artery lesions, but it is unexplored whether their diagnostic performance might be altered in patients with diabetes.
We performed a post-hoc analysis of the CONTRAST study, which prospectively enrolled an international cohort of patients undergoing routine fractional flow reserve (FFR) assessment for standard indications. Paired, repeated measurements of all physiology metrics (Pd/Pa, iFR, contrast-based FFR, and FFR) were made. A central core laboratory analyzed blinded pressure tracings in a standardized fashion.
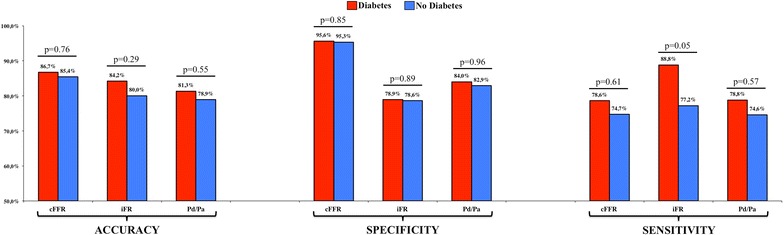
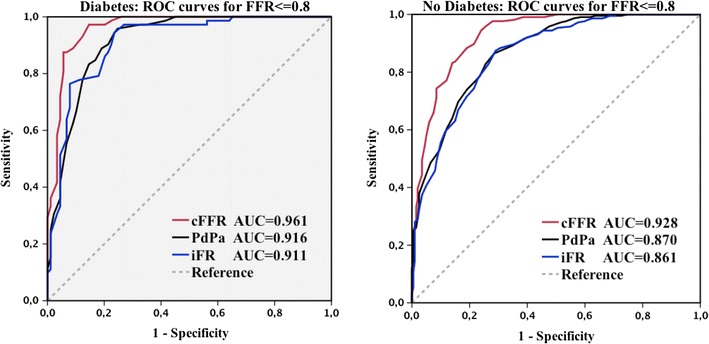
Of 763 subjects enrolled at 12 international centers, 219 (29%) had diabetes. The two groups were well-balanced for age, clinical presentation (stable or unstable), coronary vessel studied, volume and type of intracoronary contrast, and volume of intracoronary adenosine. A binary threshold of cFFR ≤ 0.83 produced an accuracy superior to both Pd/Pa and iFR when compared with FFR ≤ 0.80 in the absence of significant interaction with diabetes status; indeed, accuracy in subgroups of patients with or without diabetes was similar for cFFR (86.7 vs 85.4% respectively; p = 0.76), iFR (84.2 vs 80.0%, p = 0.29) and Pd/Pa (81.3 vs 78.9%, p = 0.55). There was no significant heterogeneity between patients with or without diabetes in terms of sensitivity and specificity of all metrics. The area under the receiver operating characteristic (ROC) curve was largest for cFFR compared with Pd/Pa and iFR which were equivalent (cFFR 0.961 and 0.928; Pd/Pa 0.916 and 0.870; iFR 0.911 and 0.861 in diabetic and non-diabetic patients respectively).
cFFR provides superior diagnostic performance compared with Pd/Pa or iFR for predicting FFR irrespective of diabetes (clinicaltrials.gov identifier NCT02184117).
无腺苷冠状动脉压力导丝指标已被提出用于检测冠状动脉病变的功能意义,但糖尿病患者中其诊断性能是否会改变尚不清楚。
我们对CONTRAST研究进行了事后分析,该研究前瞻性纳入了一组因标准适应症接受常规血流储备分数(FFR)评估的国际患者队列。对所有生理指标(Pd/Pa、iFR、基于造影剂的FFR和FFR)进行配对重复测量。一个核心实验室以标准化方式分析盲法压力描记图。
在12个国际中心登记的763名受试者中,219名(29%)患有糖尿病。两组在年龄、临床表现(稳定或不稳定)、研究的冠状动脉血管、冠状动脉造影剂的体积和类型以及冠状动脉腺苷的体积方面均衡良好。当与FFR≤0.80相比时,cFFR≤0.83的二元阈值产生的准确性优于Pd/Pa和iFR,且与糖尿病状态无显著交互作用;事实上,cFFR在糖尿病患者和非糖尿病患者亚组中的准确性相似(分别为86.7%和85.4%;p = 0.76),iFR(84.2%和80.0%,p = 0.29)和Pd/Pa(81.3%和78.9%,p = 0.55)。在所有指标的敏感性和特异性方面,糖尿病患者和非糖尿病患者之间没有显著异质性。与Pd/Pa和iFR相比,cFFR的受试者操作特征(ROC)曲线下面积最大,而Pd/Pa和iFR相当(糖尿病患者和非糖尿病患者中cFFR分别为0.961和0.928;Pd/Pa分别为0.916和0.870;iFR分别为0.911和0.861)。
与Pd/Pa或iFR相比,cFFR在预测FFR方面具有更好的诊断性能,且不受糖尿病影响(clinicaltrials.gov标识符NCT02184117)。