Lorenz Martin, Lawson Francesca, Owens David, Raccah Denis, Roy-Duval Christine, Lehmann Anne, Perfetti Riccardo, Blonde Lawrence
R&D Diabetes Division, Sanofi-Aventis Deutschland GmbH, Industrial Park Höchst, Bldg. H831, 65926, Frankfurt am Main, Germany.
R&D Diabetes Division, Sanofi, Bridgewater, NJ, USA.
Cardiovasc Diabetol. 2017 Jan 13;16(1):6. doi: 10.1186/s12933-016-0490-6.
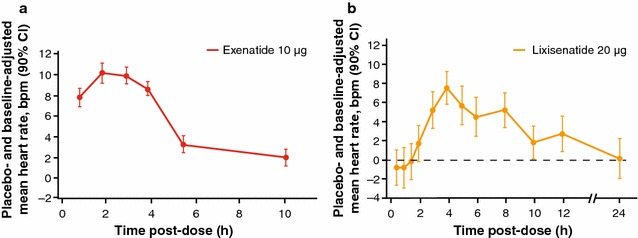
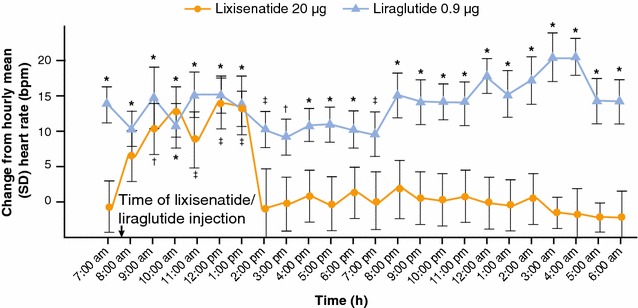
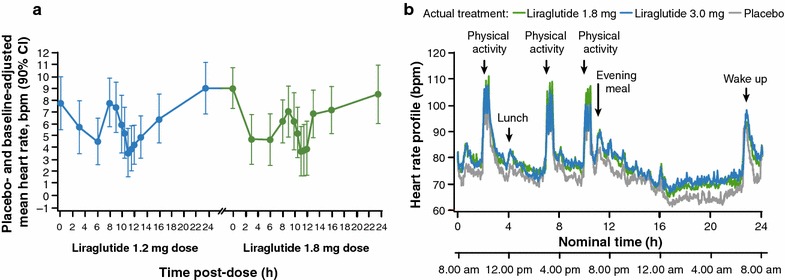
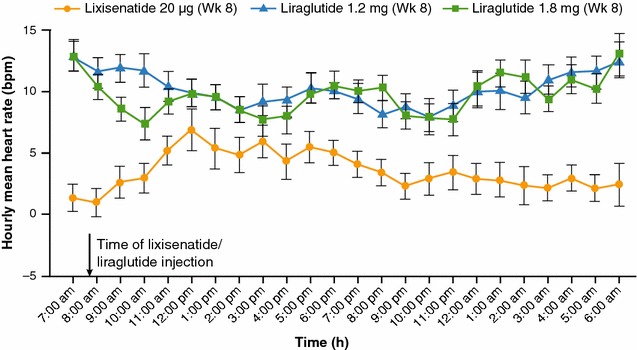
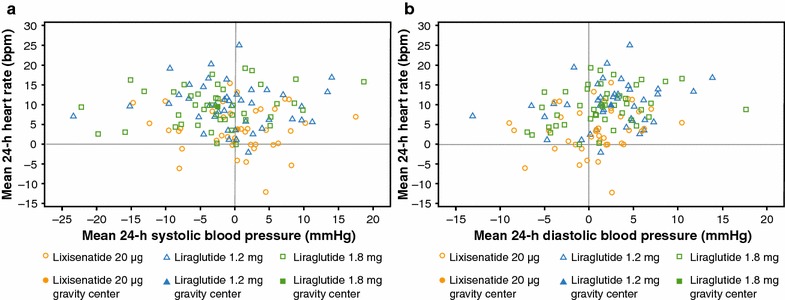
While glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are known to increase heart rate (HR), it is insufficiently recognized that the extent varies greatly between the various agonists and is affected by the assessment methods employed. Here we review published data from 24-h time-averaged HR monitoring in healthy individuals and subjects with type 2 diabetes mellitus (T2DM) treated with either short-acting GLP-1 RAs, lixisenatide or exenatide, or long-acting GLP-1 RAs, exenatide LAR, liraglutide, albiglutide, or dulaglutide (N = 1112; active-treatment arms). HR effects observed in two independent head-to-head trials of lixisenatide and liraglutide (N = 202; active-treatment arms) are also reviewed. Short-acting GLP-1 RAs, exenatide and lixisenatide, are associated with a transient (1-12 h) mean placebo- and baseline-adjusted 24-h HR increase of 1-3 beats per minute (bpm). Conversely, long-acting GLP-1 RAs are associated with more pronounced increases in mean 24-h HR; the highest seen with liraglutide and albiglutide at 6-10 bpm compared with dulaglutide and exenatide LAR at 3-4 bpm. For both liraglutide and dulaglutide, HR increases were recorded during both the day and at night. In two head-to-head comparisons, a small, transient mean increase in HR from baseline was observed with lixisenatide; liraglutide induced a substantially greater increase that remained significantly elevated over 24 h. The underlying mechanism for increased HR remains to be elucidated; however, it could be related to a direct effect at the sinus node and/or stimulation of the sympathetic nervous system, with this effect related to the duration of action of the respective GLP-1 RAs. In conclusion, this review indicates that the effects on HR differ within the class of GLP-1 RAs: short-acting GLP-1 RAs are associated with a modest and transient HR increase before returning to baseline levels, while some long-acting GLP-1 RAs are associated with a more pronounced and sustained increase during the day and night. Findings from recently completed trials indicate that a GLP-1 RA-induced increase in HR, regardless of magnitude, does not present an increased cardiovascular risk for subjects with T2DM, although a pronounced increase in HR may be associated with adverse clinical outcomes in those with advanced heart failure.
虽然已知胰高血糖素样肽-1受体激动剂(GLP-1 RAs)会增加心率(HR),但人们对不同激动剂之间这种增加程度差异很大以及受所用评估方法影响这一点认识不足。在此,我们回顾了健康个体以及接受短效GLP-1 RAs(利司那肽或艾塞那肽)或长效GLP-1 RAs(艾塞那肽长效释放制剂、利拉鲁肽、阿必鲁肽或度拉糖肽)治疗的2型糖尿病(T2DM)患者24小时平均心率监测的已发表数据(N = 1112;活性治疗组)。还回顾了利司那肽和利拉鲁肽两项独立的头对头试验(N = 202;活性治疗组)中观察到的心率影响。短效GLP-1 RAs艾塞那肽和利司那肽与安慰剂和基线调整后的24小时平均心率短暂(1 - 12小时)增加1 - 3次/分钟(bpm)相关。相反,长效GLP-1 RAs与24小时平均心率更显著增加相关;利拉鲁肽和阿必鲁肽最高可达6 - 10 bpm,而度拉糖肽和艾塞那肽长效释放制剂为3 - 4 bpm。对于利拉鲁肽和度拉糖肽,白天和夜间均记录到心率增加。在两项头对头比较中,利司那肽观察到从基线开始心率有小幅度、短暂的平均增加;利拉鲁肽引起的增加幅度大得多,且在24小时内仍显著升高。心率增加的潜在机制仍有待阐明;然而,这可能与窦房结的直接作用和/或交感神经系统的刺激有关,这种作用与各自GLP-1 RAs的作用持续时间有关。总之,本综述表明GLP-1 RAs类别中对心率的影响有所不同:短效GLP-1 RAs与心率适度且短暂增加相关,之后恢复到基线水平,而一些长效GLP-1 RAs与白天和夜间更显著且持续的增加相关。最近完成试验的结果表明,GLP-1 RA引起的心率增加,无论幅度如何,对T2DM患者而言并未增加心血管风险,尽管心率显著增加可能与晚期心力衰竭患者的不良临床结局相关。