Afonso Anoushka, Oskar Sabine, Tan Kay See, Disa Joseph J, Mehrara Babak J, Ceyhan Jihan, Dayan Joseph H
New York, N.Y.
From the Departments of Anesthesiology and Critical Care, Epidemiology and Biostatistics, Plastic and Reconstructive Surgery, and Nursing, Memorial Sloan Kettering Cancer Center.
Plast Reconstr Surg. 2017 May;139(5):1053-1061. doi: 10.1097/PRS.0000000000003235.
At present, there are limited data available regarding the use and feasibility of enhanced recovery pathways for patients undergoing microsurgical breast reconstruction. The authors sought to assess patient outcomes before and after the introduction of an enhanced recovery pathway that was adopted at a single cancer center.
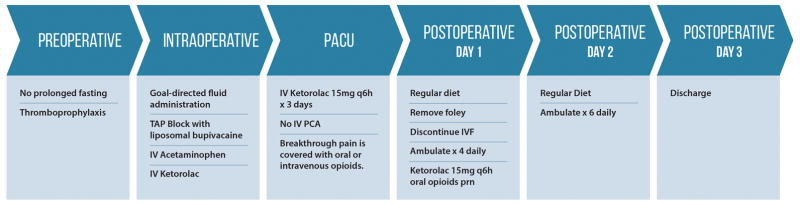
A multidisciplinary enhanced recovery pathway was developed for patients undergoing deep inferior epigastric perforator or free transverse rectus abdominis myocutaneous flap breast reconstruction. Core elements of the enhanced recovery pathway included substituting intravenous patient-controlled analgesia with ketorolac and transversus abdominis plane blocks using liposomal bupivacaine, as well as intraoperative goal-directed fluid management. Patients who underwent surgery between April and August of 2015 using the enhanced recovery pathway were compared with a historical control cohort. The primary endpoints were hospital length of stay and total postoperative opioid consumption.
In total, 91 consecutive patients were analyzed (enhanced recovery pathway, n = 42; pre-enhanced recovery pathway, n = 49). Mean hospital length of stay was significantly shorter in the enhanced recovery pathway group than in the pre-enhanced recovery pathway group (4.0 days versus 5.0 days; p < 0.0001). Total postoperative morphine equivalent consumption was also lower in the enhanced recovery pathway group (46.0 mg versus 70.5 mg; p = 0.003). There was no difference in the incidence of 30-day complications between the groups (p = 0.6).
The adoption of an enhanced recovery pathway for deep inferior epigastric perforator and transverse rectus abdominis myocutaneous flap reconstruction by multiple surgeons significantly decreased opioid consumption and reduced length of stay by 1 day.
CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, III.
目前,关于接受显微外科乳房重建手术患者的加速康复路径的应用及可行性的数据有限。作者试图评估在单一癌症中心采用加速康复路径前后的患者预后。
为接受腹壁下深动脉穿支皮瓣或游离腹直肌肌皮瓣乳房重建手术的患者制定了多学科加速康复路径。加速康复路径的核心要素包括用酮咯酸替代静脉自控镇痛以及使用脂质体布比卡因进行腹横肌平面阻滞,还有术中目标导向性液体管理。将2015年4月至8月间采用加速康复路径进行手术的患者与一个历史对照队列进行比较。主要终点指标为住院时间和术后阿片类药物总消耗量。
总共分析了91例连续患者(加速康复路径组,n = 42;加速康复路径前组,n = 49)。加速康复路径组的平均住院时间显著短于加速康复路径前组(4.0天对5.0天;p < 0.0001)。加速康复路径组术后吗啡当量总消耗量也较低(46.0毫克对70.5毫克;p = 0.003)。两组间30天并发症发生率无差异(p = 0.6)。
多名外科医生对腹壁下深动脉穿支皮瓣和腹直肌肌皮瓣重建采用加速康复路径,显著减少了阿片类药物消耗,并使住院时间缩短了1天。
临床问题/证据级别:治疗性,III级。