Cassidy Richard J, Switchenko Jeffrey M, Jegadeesh Naresh, Sayan Mutlay, Ferris Matthew J, Eaton Bree R, Higgins Kristin A, Wadsworth Jeffrey T, Magliocca Kelly R, Saba Nabil F, Beitler Jonathan J
Department of Radiation Oncology, Emory University, Atlanta, Georgia2Winship Cancer Institute at Emory University, Atlanta, Georgia.
Winship Cancer Institute at Emory University, Atlanta, Georgia3Department of Biostatistics and Bioinformatics, Emory University, Atlanta, Georgia.
JAMA Otolaryngol Head Neck Surg. 2017 Apr 1;143(4):382-388. doi: 10.1001/jamaoto.2016.3795.
The indications for adjuvant therapy in resected oral tongue cancers are based on both clinical and pathological factors, with clear evidence for adjuvant radiation in patients with pathologically positive neck lymph nodes, positive margins, and extracapsular extension, but the data for patients with no nodal disease are sparse.
To investigate determinants of failure and survival in patients with node-negative oral tongue cancer.
DESIGN, SETTING, AND PARTICIPANTS: Medical records for patients with oral tongue cancer treated with definitive surgery from 2003 to 2013 were reviewed. All patients were cN0 negative and classified as pathologically node-negative (pN0) if a neck dissection was performed. Patients received adjuvant radiotherapy (RT) or chemoradiotherapy (CRT) based on standard clinical and pathological determinants.
Kaplan-Meier and multivariable (MVA) logistic regression and Cox proportional hazard regression analyses were performed to identify patient, tumor, and treatment characteristics predictive of locoregional control (LRC) and overall survival (OS).
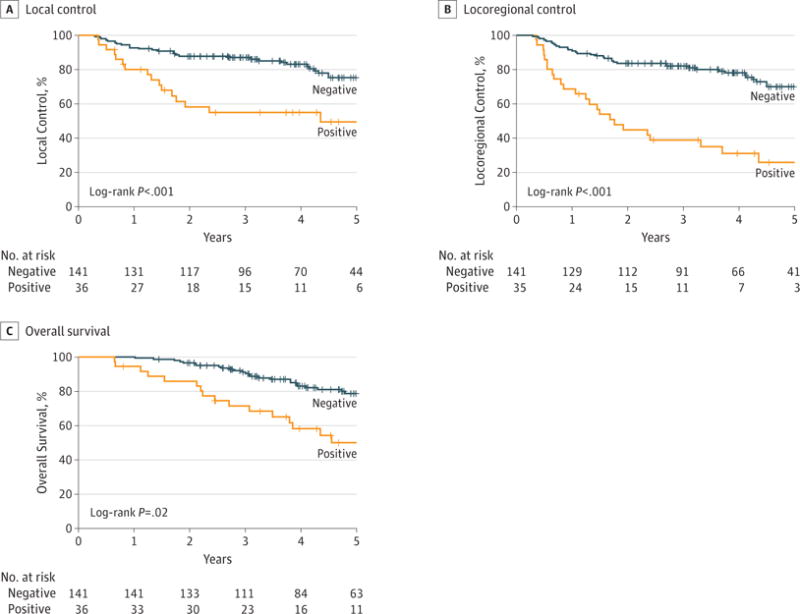
A total of 180 patients met entry criteria, with a median follow-up time of 4.9 years (range, 0.9-12.5 years); 102 patients (56.7%) were female and 42 patients (23.3%) were younger than 45 years at diagnosis. One hundred fifty-three patients (85%) had T1/T2 tumors, and 112 patients (62%) had elective neck dissections with confirmed pN0. Lymphovascular space invasion (LVSI) was present in 36 patients (20%). On MVA, LVSI (OR, 0.06; 95% CI, 0.02-0.19; P < .01) was associated with worse LRC. Elective neck dissection (odds ratio [OR], 2.99; 95% CI, 1.16-7.73; P = .02) and receipt of RT (OR, 7.74; 95% CI, 2.27-26.42; P < .01) were associated with improved LRC. Three-year LRC rates were significantly lower for patients with LVSI (38.8%; 95% CI, 22.8%, 54.6%) than those without LVSI (81.9%; 95% CI, 74.4%, 87.4%). On MVA, only LVSI (hazard ratio, 2.20; 95% CI, 1.19-4.06; P = .01) and age greater than 44 years (hazard ratio, 4.38; 95% CI, 1.34-14.27; P = .01) were associated with worse OS. Three-year OS rates were significantly lower in patients with LVSI (71.3%; 95% CI, 53.2%-83.4%) than those without LVSI (90.3%; 95% CI, 83.8%-94.3%).
Lymphovascular space invasion in patients with node-negative oral tongue cancer treated with upfront definitive surgery is associated with worse LRC and OS. Node-negative oral cavity cancers with LVSI warrant consideration of further adjuvant therapy, which should be further evaluated in a prospective setting.
口腔舌癌切除术后辅助治疗的指征基于临床和病理因素,对于病理颈部淋巴结阳性、切缘阳性和包膜外侵犯的患者,辅助放疗有明确证据,但无淋巴结转移患者的数据较少。
探讨无淋巴结转移的口腔舌癌患者失败和生存的决定因素。
设计、设置和参与者:回顾了2003年至2013年接受根治性手术治疗的口腔舌癌患者的病历。所有患者cN0阴性,若进行了颈部清扫术则分类为病理淋巴结阴性(pN0)。患者根据标准临床和病理决定因素接受辅助放疗(RT)或放化疗(CRT)。
进行Kaplan-Meier分析、多变量(MVA)逻辑回归和Cox比例风险回归分析,以确定预测局部区域控制(LRC)和总生存(OS)的患者、肿瘤和治疗特征。
共有180例患者符合纳入标准,中位随访时间为4.9年(范围0.9 - 12.5年);102例患者(56.7%)为女性,42例患者(23.3%)诊断时年龄小于45岁。153例患者(85%)患有T1/T2肿瘤,112例患者(62%)进行了选择性颈部清扫术且病理证实为pN0。36例患者(20%)存在淋巴管血管间隙侵犯(LVSI)。在多变量分析中,LVSI(比值比[OR],0.06;95%置信区间[CI],0.02 - 0.19;P < 0.01)与较差的LRC相关。选择性颈部清扫术(比值比[OR],2.99;95% CI,1.16 - 7.73;P = 0.02)和接受放疗(OR,7.74;95% CI,2.27 - 26.42;P < 0.01)与改善的LRC相关。有LVSI的患者3年LRC率(38.8%;95% CI,22.8%,54.6%)显著低于无LVSI的患者(81.9%;95% CI,74.4%,87.4%)。在多变量分析中,只有LVSI(风险比,2.20;95% CI,1.19 - 4.06;P = 0.01)和年龄大于44岁(风险比,4.38;95% CI,1.34 - 14.27;P = 0.01)与较差的OS相关。有LVSI的患者3年OS率(71.3%;95% CI,53.2% - 83.4%)显著低于无LVSI的患者(90.3%;95% CI,83.8% - 94.3%)。
接受 upfront 根治性手术治疗的无淋巴结转移口腔舌癌患者的淋巴管血管间隙侵犯与较差的LRC和OS相关。有LVSI的无淋巴结转移口腔癌值得考虑进一步的辅助治疗,应在前瞻性研究中进一步评估。