Roeder Falk, Krempien Robert
Department of Radiation Oncology, University Hospital of Munich (LMU), Marchioninistr. 15, 81377, Munich, Germany.
Clinical Cooperation Unit Molecular Radiation Oncology, German Cancer Research Center (DKFZ), Heidelberg, Germany.
Radiat Oncol. 2017 Jan 19;12(1):20. doi: 10.1186/s13014-016-0751-2.
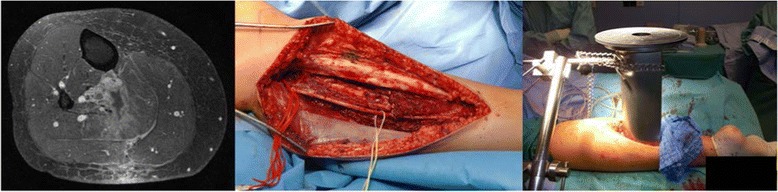
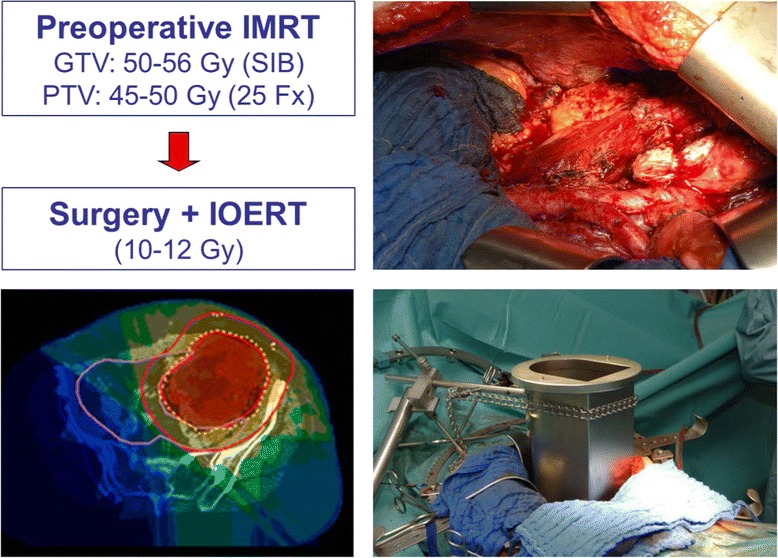
Soft-tissue sarcoma (STS) represent a rare tumor entity, accounting for less than 1% of adult malignancies. The cornerstone of curative intent treatment is surgery with free margins, although the extent of the surgical approach has been subject to change in the last decades. Multimodal approaches usually including radiation therapy have replaced extensive surgical procedures in order to preserve functionality while maintaining adequate local control. However, the possibility to apply adequate radiation doses by external beam radiation therapy (EBRT) can be limited in some situation especially in case of directly adjacent organs at risk with low radiation tolerance. Application of at least a part of the total dose via intraoperative radiation therapy (IORT) with a single fraction during the surgical procedure may overcome those limitations, because radiosensitive structures can be moved out of the radiation field resulting in reduced toxicity while the enhanced biological effectivity of the high single dose improves local control. The current review summarizes rationale, techniques, oncological and functional outcomes including possible pitfalls and associated toxicities based on the published literature for IORT focusing on extremity and retroperitoneal STS. In extremity STS, combination of limb-sparing surgery, IORT and pre- or postoperative EBRT with moderate doses consistently achieved excellent local control rates at least comparable to approaches using EBRT alone but usually including patient cohorts with higher proportions of unfavourable prognostic factors. Further on, IORT containing approaches resulted in very high limb preservation rates and good functional outcome, probably related to the smaller high dose volume. In retroperitoneal STS, the combination of preoperative EBRT, surgery and IORT consistently achieved high local control rates which seem superior to surgery alone or surgery with EBRT at least with regard to local control and in some reports even to overall survival. Further on, preoperative EBRT in combination with IORT seems to be superior to the opposite combination with regard to local control and toxicity. No major differences in wound healing disturbances or postoperative complication rates can be observed with IORT compared to non-IORT containing approaches. Neuropathy of major nerves remains a dose limiting toxicity requiring dose restrictions or exclusion from target volume. Gastrointestinal structures and ureters should be excluded from the IORT area whenever possible and the IORT volume should be restricted to the available minimum. Nevertheless, IORT represents an ideal boosting method if combined with EBRT and properly executed by experiences users which should be further evaluated preferably in prospective randomized trials.
软组织肉瘤(STS)是一种罕见的肿瘤类型,占成人恶性肿瘤的比例不到1%。根治性治疗的基石是手术切缘阴性,尽管在过去几十年中手术方式的范围有所变化。多模式治疗方法通常包括放射治疗,已取代了广泛的外科手术,以在保持足够的局部控制的同时保留功能。然而,在某些情况下,尤其是在直接相邻的低放射耐受性危险器官的情况下,通过外照射放疗(EBRT)施加足够放射剂量的可能性可能会受到限制。在手术过程中通过术中放疗(IORT)单次给予至少一部分总剂量可能会克服这些限制,因为放射敏感结构可以移出辐射野,从而降低毒性,而高单次剂量增强的生物学有效性可改善局部控制。本综述基于已发表的关于IORT的文献,总结了其原理、技术、肿瘤学和功能结果,包括可能的陷阱和相关毒性,重点关注肢体和腹膜后STS。在肢体STS中,保肢手术、IORT与中等剂量的术前或术后EBRT相结合,始终能取得优异的局部控制率,至少与单独使用EBRT的方法相当,但通常纳入的患者队列中不良预后因素的比例更高。此外,包含IORT的方法导致了非常高的肢体保留率和良好的功能结果,这可能与较小的高剂量体积有关。在腹膜后STS中,术前EBRT、手术和IORT相结合始终能取得高局部控制率,至少在局部控制方面似乎优于单纯手术或手术联合EBRT,在一些报告中甚至优于总生存率。此外,术前EBRT与IORT联合在局部控制和毒性方面似乎优于相反的联合方式。与不包含IORT的方法相比,IORT在伤口愈合障碍或术后并发症发生率方面没有观察到重大差异。主要神经的神经病变仍然是一种剂量限制性毒性,需要限制剂量或将其排除在靶体积之外。只要有可能,胃肠道结构和输尿管应排除在IORT区域之外,IORT体积应限制在可用的最小值。然而,如果与EBRT联合并由经验丰富的使用者正确实施,IORT是一种理想的增强方法,应在前瞻性随机试验中进一步评估。