Zachou Kalliopi, Arvaniti Pinelopi, Gatselis Nikolaos K, Azariadis Kalliopi, Papadamou Georgia, Rigopoulou Eirini, Dalekos George N
Department of Medicine and Research Laboratory of Internal Medicine, School of Medicine, University of Thessaly, Larissa, Greece.
Mediterr J Hematol Infect Dis. 2017 Jan 1;9(1):e2017003. doi: 10.4084/MJHID.2017.003. eCollection 2017.
BACKGROUND & OBJECTIVES: In the past, patients with haemoglobinopathies were at high risk of acquiring hepatitis C virus (HCV) due to multiple transfusions before HCV screening. In these patients, the coexistence of haemochromatosis and chronic hepatitis C (CHC) often leads to more severe liver disease. We assessed the HCV prevalence, clinical characteristics and outcome in this setting with particular attention to the response to treatment including therapies with the new direct acting antivirals (DAAs).
The medical records of 81 consecutive patients followed the last 15 years were reviewed retrospectively.
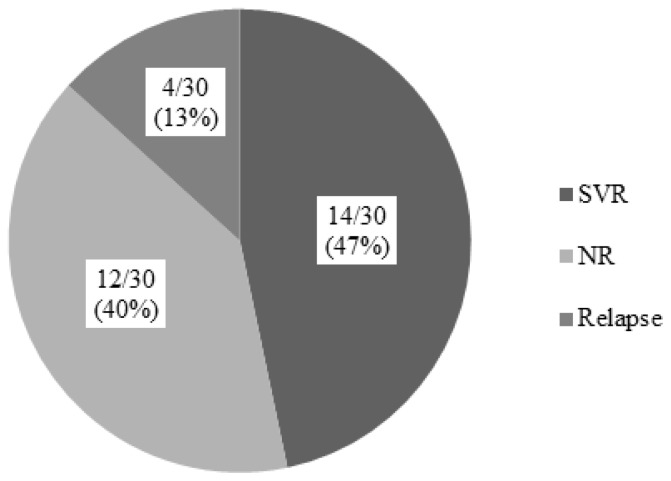
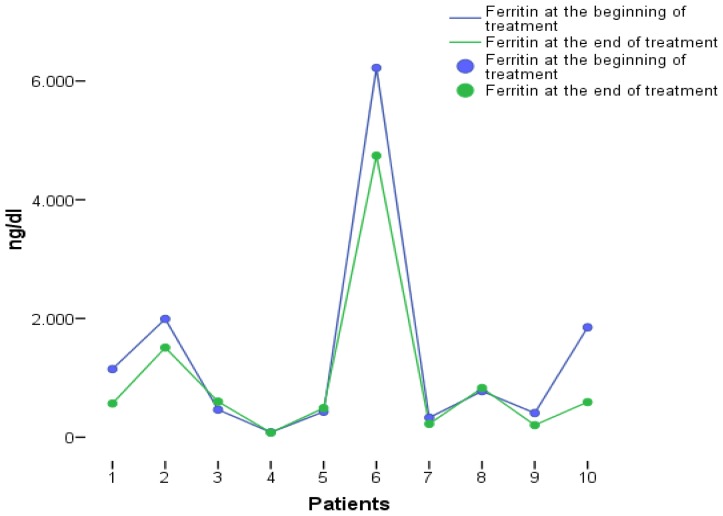
43/81 (53%) patients were anti-HCV positive including 31/43 (72.1%) with CHC (HCV-RNA positive; age 25±7 years; 45.2% with genotype 1b; 19.4% cirrhotics; baseline ferritin 887 ng/ml; range: 81-10.820). Thirty patients received IFN-based therapy with or without ribavirin with sustained virological response (SVR) in 14/30 (46.7%). Eleven patients (9 non-responders to IFN-based therapies, one in relapse and one naïve) received treatment with DAAs (SVR: 100%). 3/11 patients increased their transfusion needs while 1/11 reported mild arthralgias. No drug-drug interactions between DAAs and chelation agents were observed as attested by the stability of ferritin levels during treatment.
More than 1/3 of patients with haemoglobinopathies suffered from CHC. Response rates to IFN-based treatment seem to be similar to other patients with CHC, while most importantly, treatment with DAAs was excellent and safe even in difficult to treat patients (most null responders with severe fibrosis) suggesting that this group of HCV patients should no longer be regarded as a difficult to treat.
过去,由于在丙型肝炎病毒(HCV)筛查前多次输血,血红蛋白病患者感染HCV的风险很高。在这些患者中,血色素沉着症与慢性丙型肝炎(CHC)共存往往会导致更严重的肝脏疾病。我们评估了这种情况下的HCV患病率、临床特征及预后,特别关注对治疗的反应,包括使用新型直接作用抗病毒药物(DAA)的治疗。
回顾性分析了过去15年连续随访的81例患者的病历。
81例患者中有43例(53%)抗HCV阳性,其中31例(72.1%)为CHC(HCV-RNA阳性;年龄25±7岁;45.2%为1b型基因型;19.4%为肝硬化患者;基线铁蛋白887 ng/ml;范围:81-10,820)。30例患者接受了含或不含利巴韦林的基于干扰素的治疗,14例(46.7%)获得持续病毒学应答(SVR)。11例患者(9例对基于干扰素的治疗无应答者、1例复发患者和1例初治患者)接受了DAA治疗(SVR:100%)。11例患者中有3例输血需求增加,1例报告有轻度关节痛。治疗期间铁蛋白水平稳定,证明未观察到DAA与螯合剂之间的药物相互作用。
超过1/3的血红蛋白病患者患有CHC。基于干扰素的治疗应答率似乎与其他CHC患者相似,而最重要的是,即使在难治性患者(大多数无应答且有严重纤维化的患者)中,DAA治疗效果良好且安全,这表明这组HCV患者不应再被视为难治性患者。