Steppich Birgit, Groha Philip, Ibrahim Tareq, Schunkert Heribert, Laugwitz Karl-Ludwig, Hadamitzky Martin, Kastrati Adnan, Ott Ilka
Deutsches Herzzentrum der Technischen Universität München, Lazarettstr. 36, 80636, Munich, Germany.
Medizinische Klinik Klinikum rechts der Isar der Technischen Universität München, Ismaningerstr. 22, 81675, Munich, Germany.
BMC Cardiovasc Disord. 2017 Jan 21;17(1):38. doi: 10.1186/s12872-016-0464-3.
Erythropoietin (EPO) has been suggested to promote cardiac repair after MI. However, the randomized, double-blind, placebo controlled REVIVAL-3 trial showed that short term high dose EPO in timely reperfused myocardium does not improve left ventricular ejection fraction after 6 months. Moreover, the study raised safety concerns due to a trend towards a higher incidence of adverse clinical events as well as a increase in neointima formation after treatment with EPO. The present study therefore aimed to assess the 5-year clinical outcomes.
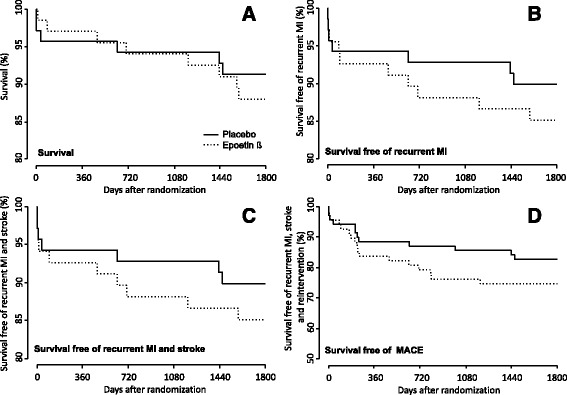
After successful reperfusion 138 patients with STEMI were randomly assigned to receive epoetin beta (3.33×10 U, n = 68) or placebo (n = 70) immediately, 24 and 48 h after percutaneous coronary intervention. The primary outcome of the present study- the combined incidence of MACE 5 years after randomization - occurred in 25% of the patients assigned to epoetin beta and 17% of the patients assigned to placebo (RR 1.5; 95% CI 0.8-3.5; p = 0.26). Target lesion revascularization was required in 15 patients (22.1%) treated with epoetin-ß and 9 patients (12.9%) treated with placebo (p = 0.15). Analysis of patients in the upper and lower quartile of baseline hemoglobin as an indirect estimate of endogenous erythropoietin levels revealed no significant impact of endogenous erythropoietin on efficiency of exogen administered epoetin-ß in terms of death and MACE.
These long-term follow-up data show that epoetin beta does not improve clinical outcomes of patients with acute myocardial infarction.
URL www.clinicaltrials.gov ; Unique identifier NCT00390832; trial registration date October 19th 2006.
促红细胞生成素(EPO)被认为可促进心肌梗死后的心脏修复。然而,随机、双盲、安慰剂对照的REVIVAL - 3试验表明,在及时再灌注的心肌中短期高剂量使用EPO,6个月后左心室射血分数并未改善。此外,该研究引发了对安全性的担忧,因为临床不良事件发生率有升高趋势,且EPO治疗后新生内膜形成增加。因此,本研究旨在评估5年的临床结局。
138例ST段抬高型心肌梗死患者在经皮冠状动脉介入治疗成功再灌注后,随机分为立即、24小时和48小时接受促红细胞生成素β(3.33×10单位,n = 68)或安慰剂(n = 70)治疗。本研究的主要结局——随机分组后5年主要不良心血管事件(MACE)的合并发生率,在接受促红细胞生成素β治疗的患者中为25%,在接受安慰剂治疗的患者中为17%(风险比1.5;95%置信区间0.8 - 3.5;p = 0.26)。接受促红细胞生成素β治疗的15例患者(22.1%)和接受安慰剂治疗的9例患者(12.9%)需要进行靶病变血管重建(p = 0.15)。将基线血红蛋白处于上四分位数和下四分位数的患者作为内源性促红细胞生成素水平的间接估计进行分析,结果显示内源性促红细胞生成素在外源性促红细胞生成素β治疗的死亡和MACE方面对其疗效无显著影响。
这些长期随访数据表明,促红细胞生成素β不能改善急性心肌梗死患者的临床结局。
网址www.clinicaltrials.gov;唯一标识符NCT00390832;试验注册日期2006年10月19日。