He Huan, Xu Hailin, Lu Hao, Dang Yu, Huang Wei, Zhang Qing
Department of Orthopaedics, Jiangyou 903 Hospital, Mianyang No. 9 Huafengxincun, Jiangyou, Sichuan, 621700, China.
Department of Trauma and Orthopaedics, People's Hospital, Peking University, South Xizhimen Street No. 11, Beijing, Xicheng District, 100044, China.
BMC Musculoskelet Disord. 2017 Jan 23;18(1):35. doi: 10.1186/s12891-017-1413-8.
Osteoid osteoma (OO) is a common benign bone tumour that is rarely found in the talus. Its nidus is difficult to detect on early imaging. The atypical symptoms of OO and the presence of concurrent trauma or sports injuries may lead to misdiagnosis and delayed treatment. We herein analyse a case of misdiagnosis of OO of the talus and discuss how to improve the early diagnosis of this rare lesion, thereby permitting rapid treatment.
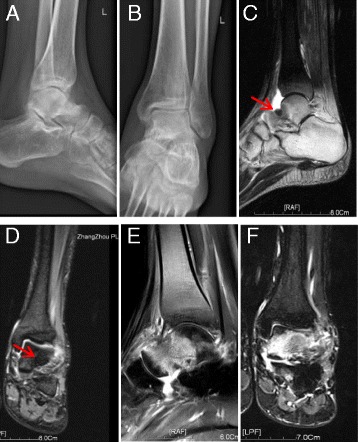
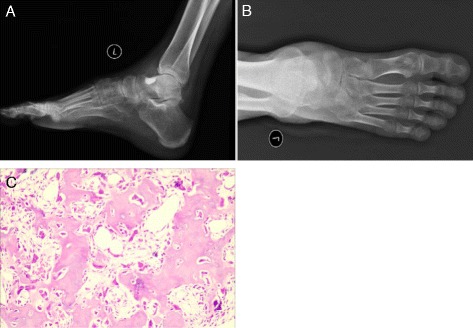
A 23-year-old man with a history of left ankle sprains and chronic pain was diagnosed with another ankle sprain and managed conservatively based on normal X-ray findings. After 1 year of recurring pain, he was diagnosed with ankle traumatic arthritis and underwent arthroscopic surgery. His preoperative ankle X-ray findings were still normal, and magnetic resonance imaging at that time demonstrated bone marrow oedema of the left talus. His symptoms reappeared shortly after surgery and progressively worsened. Magnetic resonance imaging performed 3 months after surgery demonstrated widespread bone marrow oedema of the talus. The patient presented to our hospital for pain assessment and was diagnosed with OO of the talus 3 years after his symptoms began. Preoperative computed tomography (CT) demonstrated a typical nidus of OO of the talus. After a second surgery, the patient's symptoms completely resolved, and pathologic examination confirmed that the lesion was OO. The patient recovered 3 months later and was able to walk normally.
OO of the ankle joint exhibits a progressive course and is difficult to diagnose at an early stage. Patients with OO of the talus often have atypical imaging findings, no signs of ankle instability, and no anterior talofibular ligament tenderness. CT is valuable for diagnosing OO, although multiple CT scans may be required to detect the nidus. Proper imaging helps doctors to achieve the correct diagnosis early in the disease course, significantly shortening the treatment cycle and improving the patient's quality of life.
骨样骨瘤(OO)是一种常见的良性骨肿瘤,很少见于距骨。其瘤巢在早期影像学检查中难以发现。骨样骨瘤的非典型症状以及并发创伤或运动损伤的存在可能导致误诊和治疗延迟。我们在此分析一例距骨骨样骨瘤误诊病例,并讨论如何提高对这种罕见病变的早期诊断,从而实现快速治疗。
一名有左脚踝扭伤和慢性疼痛病史的23岁男性,基于正常的X线检查结果被诊断为再次脚踝扭伤并接受保守治疗。在反复疼痛1年后,他被诊断为踝关节创伤性关节炎并接受了关节镜手术。他术前的脚踝X线检查结果仍正常,当时的磁共振成像显示左距骨骨髓水肿。术后不久他的症状再次出现并逐渐加重。术后3个月进行的磁共振成像显示距骨广泛骨髓水肿。患者因疼痛评估前来我院就诊,症状出现3年后被诊断为距骨骨样骨瘤。术前计算机断层扫描(CT)显示距骨骨样骨瘤的典型瘤巢。二次手术后,患者症状完全缓解,病理检查证实病变为骨样骨瘤。患者3个月后康复,能够正常行走。
踝关节骨样骨瘤病程呈进行性,早期难以诊断。距骨骨样骨瘤患者通常有非典型的影像学表现,无踝关节不稳定体征,无前距腓韧带压痛。CT对骨样骨瘤的诊断有价值,但可能需要多次CT扫描才能检测到瘤巢。合适的影像学检查有助于医生在病程早期做出正确诊断,显著缩短治疗周期并提高患者生活质量。