Kloos Richard T
Veracyte, Inc., Department of Medical Affairs, Senior Medical Director-Endocrinology, California, USA, Phone: +1(650)243-6300, E-mail:
Mol Imaging Radionucl Ther. 2017 Feb 9;26(Suppl 1):36-49. doi: 10.4274/2017.26.suppl.05.
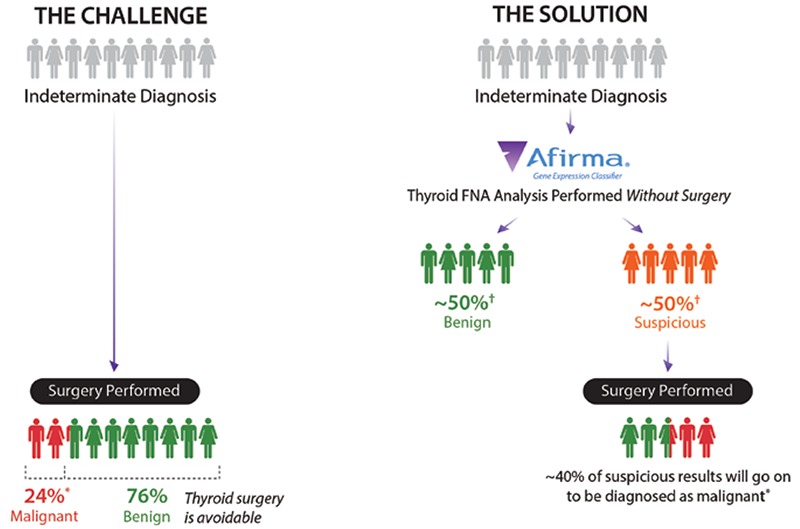
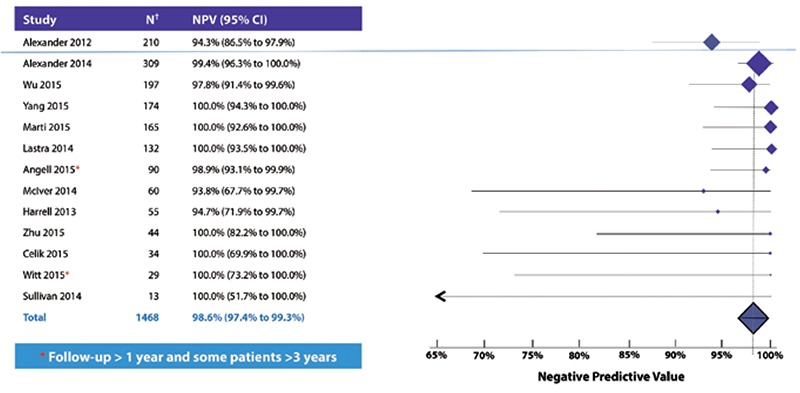
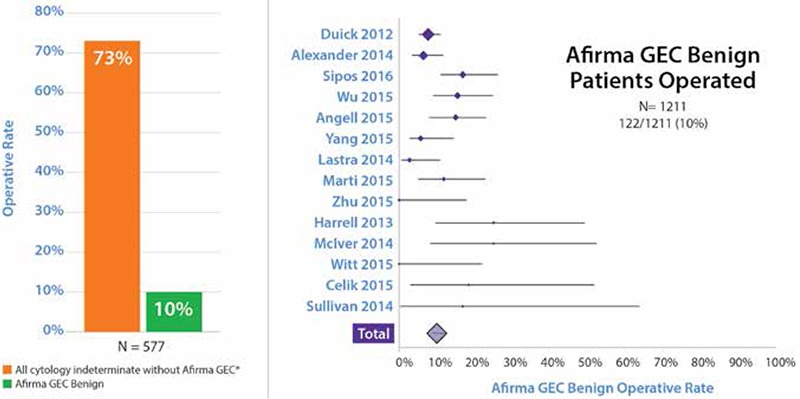
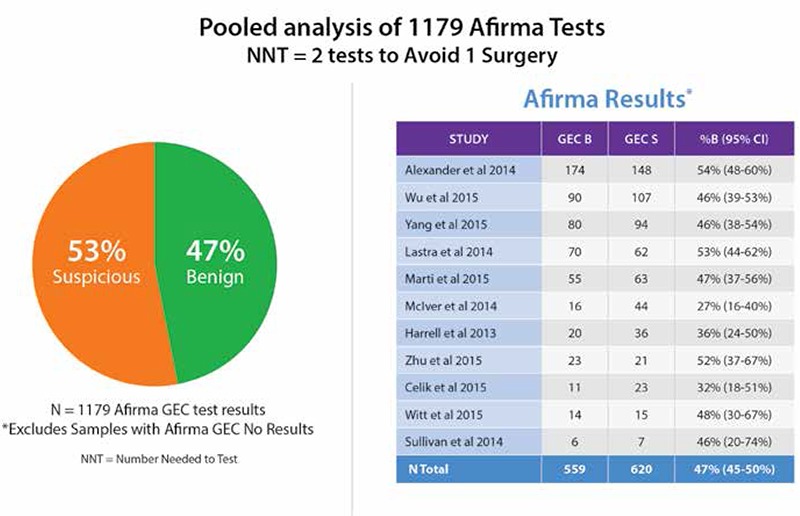
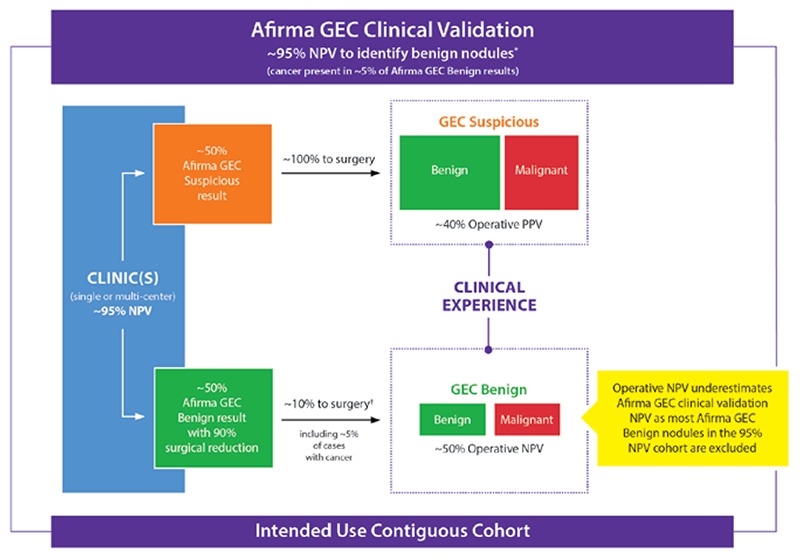
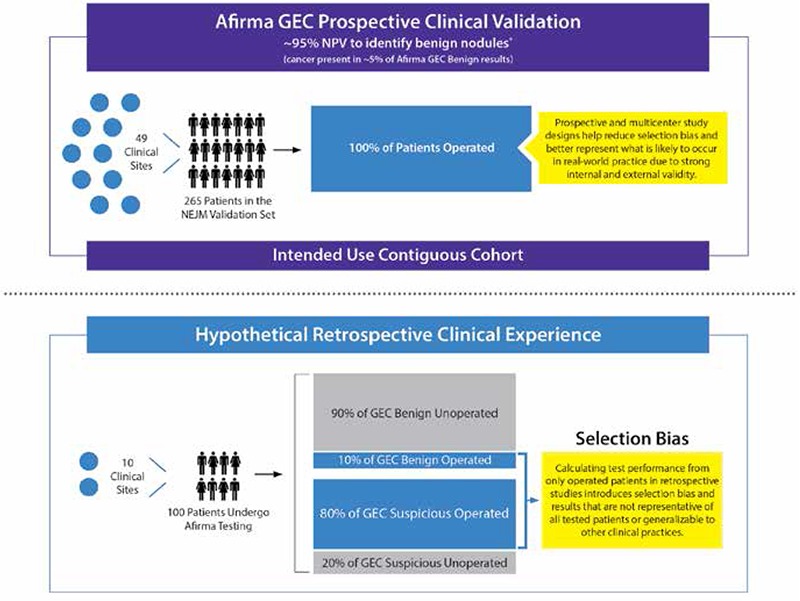
Thyroid fine-needle aspiration biopsy results are cytologically indeterminate in 15-30% of cases. When these nodules undergo diagnostic surgery, approximately three-quarters are histologically benign. These unnecessary surgeries diminish quality of life, generate complications, and increase healthcare costs. The Afirma gene expression classifier (GEC) is validated to pre-operatively identify cytologically indeterminate nodules likely to be truly benign so that surgery can be avoided. Its performance is supported by robust multicenter prospective and blinded clinical validation studies, and supported by extensive independent clinical utility publications which show a marked reduction in surgery among patients with benign Afirma GEC results. To rule-out cancer and avoid unnecessary diagnostic surgery, Afirma's quality and depth of validation stand alone. The accuracy of a benign result is the negative predictive value (NPV). Afirma achieves an NPV ≥94% among cytologically indeterminate nodules (Bethesda III or IV). Thirteen clinical utility studies describing 1468 GEC benign patients demonstrate that few Afirma GEC benign nodules undergo surgery, including after 3 years of follow-up. With a specificity of 52%, over half of the truly benign nodules with indeterminate cytology receive a benign GEC result. High test sensitivity is critical to safely rule out cancer. The Afirma GEC's 90% sensitivity means that regardless of the pre-test risk of malignancy, 90% of all malignant nodules are GEC suspicious. The Afirma GEC has transformed patient care. Where the majority of cytologically indeterminate patients were once operated to determine if the nodule was benign or malignant, now nearly half of these surgeries can be avoided.
甲状腺细针穿刺活检结果在15%至30%的病例中细胞学诊断不明确。当这些结节接受诊断性手术时,约四分之三在组织学上为良性。这些不必要的手术会降低生活质量、引发并发症并增加医疗成本。Afirma基因表达分类器(GEC)已得到验证,可在术前识别可能真正为良性的细胞学诊断不明确的结节,从而避免手术。其性能得到了强有力的多中心前瞻性和盲法临床验证研究的支持,也得到了大量独立临床效用出版物的支持,这些出版物表明,Afirma GEC结果为良性的患者手术量显著减少。为了排除癌症并避免不必要的诊断性手术,Afirma的验证质量和深度是独一无二的。良性结果的准确性即阴性预测值(NPV)。在细胞学诊断不明确的结节(贝塞斯达III级或IV级)中,Afirma的NPV≥94%。13项描述1468例GEC结果为良性患者的临床效用研究表明,很少有Afirma GEC结果为良性的结节会接受手术,包括在3年随访之后。由于特异性为52%,超过一半细胞学诊断不明确但真正为良性的结节获得了GEC良性结果。高检测灵敏度对于安全排除癌症至关重要。Afirma GEC的90%灵敏度意味着,无论术前恶性风险如何,所有恶性结节中有90%的GEC检测结果为可疑。Afirma GEC改变了患者护理模式。过去,大多数细胞学诊断不明确的患者会接受手术以确定结节是良性还是恶性,现在近一半的此类手术可以避免。