Beom Jin Ho, You Je Sung, Kim Min Joung, Seung Min Kyung, Park Yoo Seok, Chung Hyun Soo, Chung Sung Phil, Park Incheol
Department of Emergency Medicine, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, 120-752, Seoul, Republic of Korea.
Department of Emergency Medicine, Hallym University Sacred Heart Hospital, Hallym University Medical Center, Gyeonggi-Do, Republic of Korea.
Scand J Trauma Resusc Emerg Med. 2017 Jan 26;25(1):8. doi: 10.1186/s13049-017-0352-6.
The purpose of this study was to identify the relationship between the deeper and faster chest compressions suggested by the 2010 cardiopulmonary resuscitation guidelines and complications arising from chest compressions, using multi-detector computed tomography.
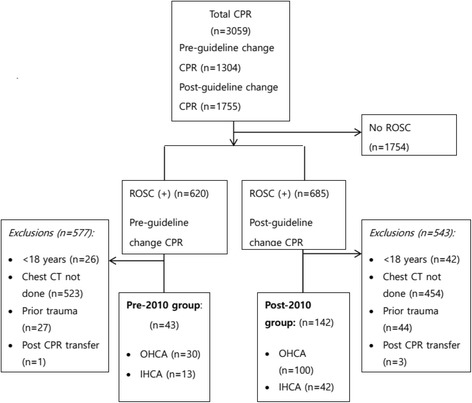
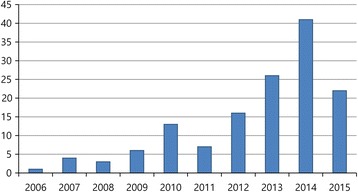
We performed a retrospective analysis of prospective registry data. This study was conducted with in- and out-of-hospital cardiac arrest patients who underwent successful resuscitation in the emergency departments of two academic tertiary care centres from October 2006 to September 2010 (pre-2010 group) and from October 2011 to September 2015 (post-2010 group). We examined chest injuries related to chest compressions, classified as follows: rib fracture, sternal fracture, and other uncommon complications.
We enrolled 185 patients in this study. The most frequent complication to occur in both groups was rib fracture: 27 (62.8%) and 112 (78.9%) patients in the pre-2010 and post-2010 groups, respectively (p = 0.03). However, we observed no statistical differences in sternum fracture, the second most common complication (p = 0.80). Retrosternal and mediastinal haematoma were not reported in the pre-2010 group but 13 patients (9.1%) in the post-2010 group were reported to have haematoma (p = 0.04). Nine serious, life-threatening complications occurred, all in the post-2010 group. Among the younger group (less than 65 years old), 8 (38.1%) patients in the pre-2010 group and 40 (64.5%) in the post-2010 group sustained rib fractures.
The deeper and faster chest compressions for enhancing ROSC are associated with increased occurrence of complications. Additional studies are needed to compensate for the limitations of our study design.
This study found that the 2010 guidelines, recommending deeper and faster chest compressions, led to an increased proportion of rib fractures and retrosternal and mediastinal haematoma.
本研究的目的是利用多排螺旋计算机断层扫描,确定2010年心肺复苏指南所建议的更深更快的胸外按压与胸外按压引起的并发症之间的关系。
我们对前瞻性登记数据进行了回顾性分析。本研究纳入了2006年10月至2010年9月(2010年前组)以及2011年10月至2015年9月(2010年后组)在两家学术性三级医疗中心急诊科成功复苏的院内心脏骤停和院外心脏骤停患者。我们检查了与胸外按压相关的胸部损伤,分类如下:肋骨骨折、胸骨骨折和其他罕见并发症。
本研究共纳入185例患者。两组中最常见的并发症都是肋骨骨折:2010年前组和2010年后组分别有27例(62.8%)和112例(78.9%)患者发生肋骨骨折(p = 0.03)。然而,我们观察到胸骨骨折(第二常见并发症)无统计学差异(p = 0.80)。2010年前组未报告胸骨后和纵隔血肿,但2010年后组有13例患者(9.1%)报告有血肿(p = 0.04)。发生了9例严重的、危及生命的并发症,均在2010年后组。在较年轻组(小于65岁)中,2010年前组有8例(38.1%)患者和2010年后组有40例(64.5%)患者发生肋骨骨折。
为提高自主循环恢复而进行的更深更快的胸外按压与并发症发生率增加有关。需要进一步的研究来弥补我们研究设计的局限性。
本研究发现,2010年指南推荐的更深更快的胸外按压导致肋骨骨折以及胸骨后和纵隔血肿的比例增加。