Mimura Tomohiro, Mori Kanji, Kitagawa Masahiro, Ueki Mariko, Furuya Yuki, Kawasaki Taku, Imai Shinji
Department of Orthopedic Surgery, Shiga University of Medical Science, Tsukinowa-cho, Seta, Otsu, Shiga, 520-2192, Japan.
BMC Musculoskelet Disord. 2017 Jan 31;18(1):50. doi: 10.1186/s12891-017-1426-3.
Acetabular dysplasia (AD) is a well-known cause of osteoarthritis (OA) of the hip, with its prevalence previously determined on plain radiography. The prevalence of preexisting AD was reported as 7.3% in a patient-based Asian population. Although computed tomography (CT) could evaluate AD in multiple planes, its prevalence using multiplanar CT images has not been reported. We investigated its prevalence with CT on coronal, axial, and sagittal planes and then determined if adding the axial and sagittal planes enhanced the investigation.
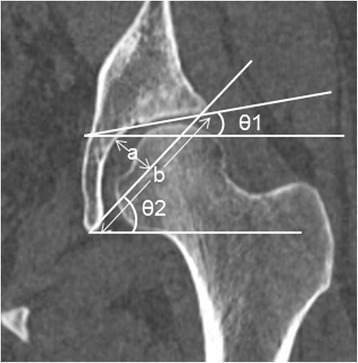
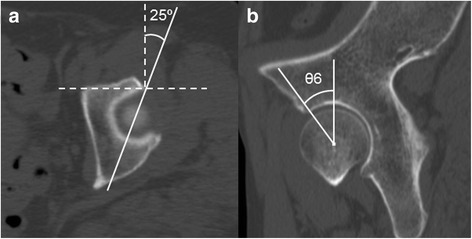
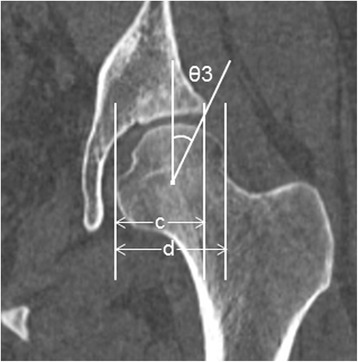
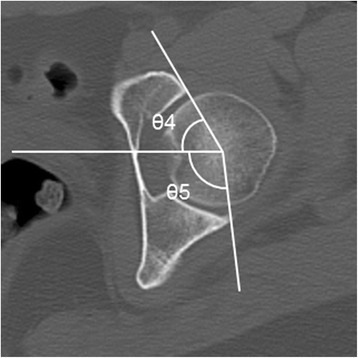
We retrospectively examined 52 consecutive Japanese individuals (mean age 59.4 years) who had undergone CT for conditions unrelated to hip disorders. The inclusion criteria of CT images were (1) reconstructed axial slice thickness of ≤1 mm and (2) normal pelvic rotations and tilt. Exclusion criteria were (1) age <20 years, (2) neither hip center could be clearly detected, (3) evidence of hip OA. The parameters used to define AD on the coronal plane were the center-edge angle, Sharp angle, acetabular index, acetabular depth ratio, and acetabulum head index. The anterior and posterior acetabular sector angles were used as axial parameters and the vertical-center-anterior margin angle as the sagittal parameter. AD prevalence was calculated using multiplanar images and then compared with the previously reported Asian prevalence using 95% confidence intervals (CI). In this study, we defined "prevalence" as the proportion of subjects who had AD in at least one hip.
The mean prevalence of AD on coronal, axial, and sagittal planes was 16.9, 15.4, and 7.7%, respectively. The lowest prevalence found by combining the three planes was 25.0% (95% CI 15.2-38.2%). This prevalence was significantly higher than that in the previously reported Asian population (7.3%).
At the lowest estimate, the prevalence of AD evaluated in three planes was more than twice as high as the previously reported prevalence in Asians when we investigated its prevalence using multiplanar images. The prevalence of AD in the axial and sagittal planes was not negligible. We therefore suggest that it is important to add axial and sagittal planes' data when investigating the prevalence of AD.
髋臼发育不良(AD)是髋关节骨关节炎(OA)的一个众所周知的病因,其患病率此前通过X线平片确定。在一个以患者为基础的亚洲人群中,既往AD的患病率报告为7.3%。尽管计算机断层扫描(CT)可以在多个平面评估AD,但其在多平面CT图像上的患病率尚未见报道。我们通过CT在冠状面、轴位和矢状面上研究其患病率,然后确定增加轴位和矢状面是否能加强研究。
我们回顾性检查了52例连续的日本个体(平均年龄59.4岁),他们因与髋关节疾病无关的情况接受了CT检查。CT图像的纳入标准为:(1)重建轴位切片厚度≤1mm;(2)骨盆旋转和倾斜正常。排除标准为:(1)年龄<20岁;(2)双侧髋关节中心均无法清晰检测到;(3)髋关节OA的证据。用于在冠状面定义AD的参数为中心边缘角、夏普角、髋臼指数、髋臼深度比和髋臼头指数。髋臼前后扇形角用作轴位参数,垂直中心前缘角用作矢状位参数。使用多平面图像计算AD患病率,然后使用95%置信区间(CI)与先前报道的亚洲患病率进行比较。在本研究中,我们将“患病率”定义为至少一侧髋关节患有AD的受试者比例。
AD在冠状面、轴位和矢状面的平均患病率分别为16.9%、15.4%和7.7%。三个平面联合发现的最低患病率为25.0%(95%CI 15.2 - 38.2%)。该患病率显著高于先前报道的亚洲人群(7.3%)。
在我们使用多平面图像研究AD患病率时,最低估计值显示,在三个平面评估的AD患病率是先前报道的亚洲人患病率的两倍多。AD在轴位和矢状面的患病率不可忽视。因此,我们建议在调查AD患病率时增加轴位和矢状面的数据很重要。