Fung Colman Siu Cheung, Wan Eric Yuk Fai, Chan Anca Ka Chun, Lam Cindy Lo Kuen
Department of Family Medicine and Primary Care, the University of Hong Kong, 3/F Ap Lei Chau Clinic, 161 Main Street, Ap Lei Chau, Hong Kong.
BMC Nephrol. 2017 Feb 2;18(1):47. doi: 10.1186/s12882-017-0468-y.
Estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) are renal markers associated with risks of cardiovascular diseases (CVD) and all-cause mortality in diabetic patients. This study aims to quantify such risks in Chinese diabetic patients based on eGFR and UACR.
This was a territory-wide retrospective cohort study on primary care diabetic patients with documented eGFR and UACR but without baseline CVD in 2008/2009. They were followed up till 2013 on CVD events and mortality. Associations between eGFR/UACR and incidence of CVD/mortality were evaluated by multivariable Cox proportional models adjusted with socio-demographic and clinical characteristics.
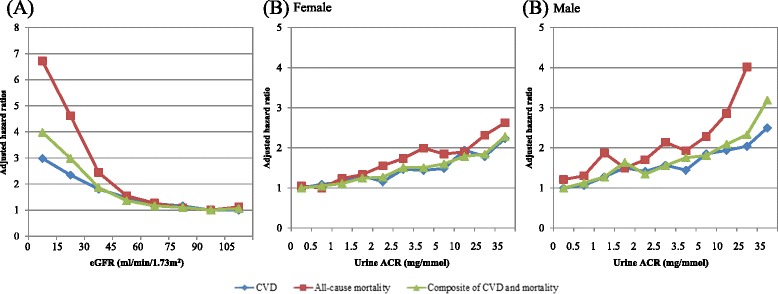
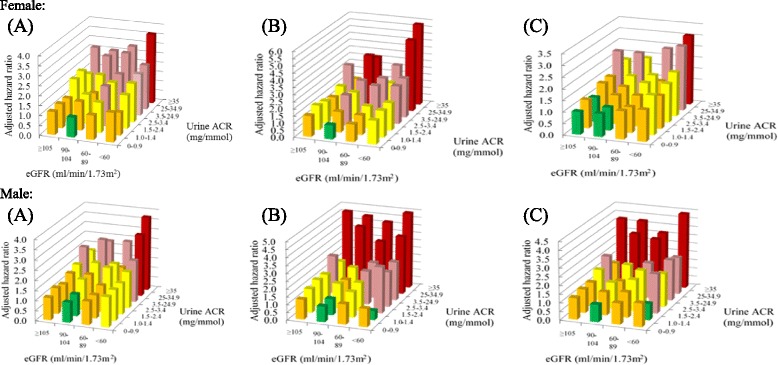
The data of 66,311 patients who had valid baseline eGFR and UACR values were analysed. The risks of CVD events and mortality increased exponentially with the decrease in eGFR, with a hazard ratio (HR) increasing from 1.63 to 4.55 for CVD, and from 1.70 to 9.49 for mortality, associated with Stage 3 to 5 CKD, compared to Stage 1 CKD. UACR showed a positive linear association with CVD events and mortality. Microalbuminuria was associated with a HR of 1.58 and 2.08 for CVD and mortality in male (1.48 and 1.79 for female), respectively, compared to no microalbuminuria. Male patients with UACR 1-1.4 mg/mmol and eGFR ≥90 ml/min/1.73 m (60-89 ml/min/1.73 m) had a HR of 1.25 (1.43) for CVD. Female patients with UACR 2.5-3.4 mg/ml and eGFR ≥90 ml/min/1.73 m (60-89 ml/min/1.73 m) had a HR of 1.45 (1.65) for CVD.
Risks of CVD events and mortality increased exponentially with eGFR drop, while UACR showed positive predictive linear relationships, and the risks started even in high-normal albuminuria. UACR-based HR was further modified according to eGFR level, with risk progressed with CKD stage. Combining eGFR and UACR level was more accurate in predicting risk of CVD/mortality. The findings call for more aggressive screening and intervention of microalbuminuria in diabetic patients.
估计肾小球滤过率(eGFR)和尿白蛋白与肌酐比值(UACR)是与糖尿病患者心血管疾病(CVD)风险及全因死亡率相关的肾脏指标。本研究旨在基于eGFR和UACR对中国糖尿病患者的此类风险进行量化。
这是一项针对2008/2009年有记录的eGFR和UACR但无基线CVD的基层医疗糖尿病患者的全地区回顾性队列研究。对他们随访至2013年,观察CVD事件和死亡率。通过对社会人口统计学和临床特征进行调整的多变量Cox比例模型评估eGFR/UACR与CVD发病率/死亡率之间的关联。
分析了66311例具有有效基线eGFR和UACR值患者的数据。CVD事件和死亡率风险随eGFR降低呈指数增加,与1期慢性肾脏病(CKD)相比,3至5期CKD患者发生CVD的风险比(HR)从1.63增至4.55,死亡风险比从1.70增至9.49。UACR与CVD事件和死亡率呈正线性关联。与无微量白蛋白尿相比,男性微量白蛋白尿患者发生CVD和死亡的HR分别为1.58和2.08(女性分别为1.48和1.79)。UACR为1 - 1.4mg/mmol且eGFR≥90ml/min/1.73m²(60 - 89ml/min/1.73m²)的男性患者发生CVD的HR为1.25(1.43)。UACR为2.5 - 3.4mg/ml且eGFR≥90ml/min/1.7m²(60 - 89ml/min/1.73m²)的女性患者发生CVD的HR为1.45(1.65)。
CVD事件和死亡率风险随eGFR下降呈指数增加,而UACR显示出正性预测线性关系,且风险在高正常蛋白尿水平时就已开始。基于UACR的HR根据eGFR水平进一步调整,风险随CKD分期进展。联合eGFR和UACR水平在预测CVD/死亡率风险方面更准确。这些发现呼吁对糖尿病患者的微量白蛋白尿进行更积极的筛查和干预。