Effoe Valery S, Wagenknecht Lynne E, Echouffo Tcheugui Justin B, Chen Haiying, Joseph Joshua J, Kalyani Rita R, Bell Ronny A, Wu Wen-Chih H, Casanova Ramon, Bertoni Alain G
Division of General Internal Medicine, Morehouse School of Medicine, Atlanta, GA
Department of Epidemiology and Prevention, Wake Forest School of Medicine, Winston Salem, NC.
J Am Heart Assoc. 2017 Feb 2;6(2):e004229. doi: 10.1161/JAHA.116.004229.
Studies exploring the association between insulin resistance (IR) and cardiovascular disease in blacks have not been conclusive, especially for coronary heart disease (CHD). The McAuley index and homeostasis model assessment of IR (HOMA-IR) perform differently in predicting cardiovascular disease. We investigated this association in the Jackson Heart Study, a large longitudinal cohort of blacks.
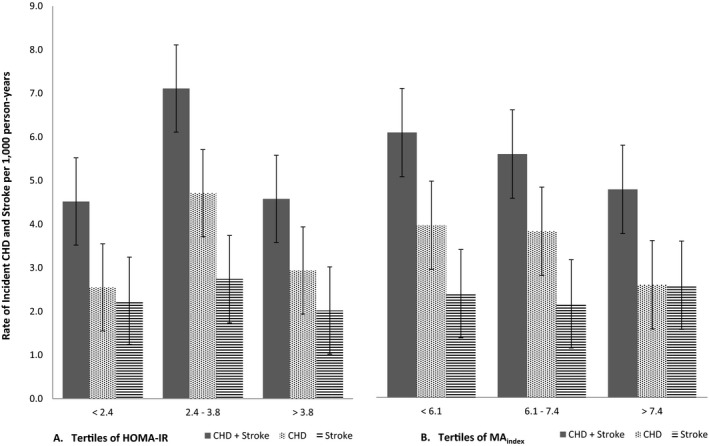
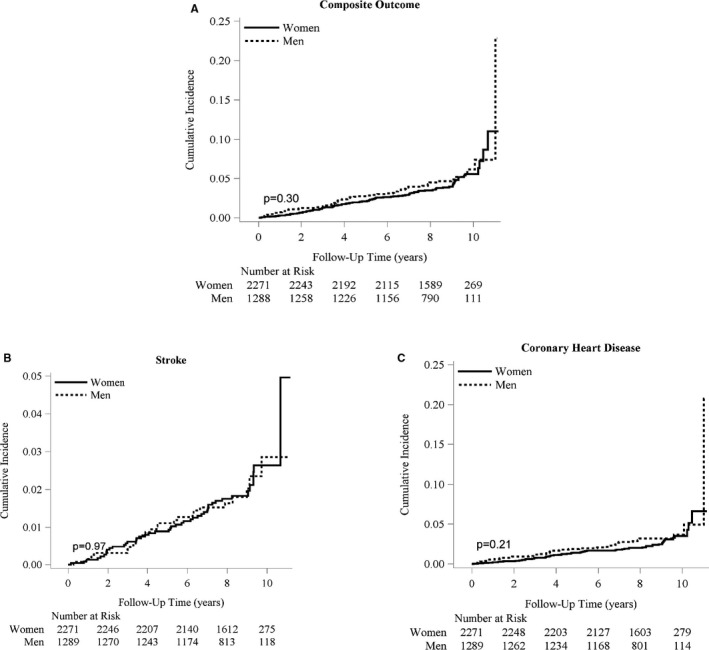
IR was estimated for 3565 participants without diabetes mellitus and cardiovascular disease at baseline using the McAuley index and HOMA-IR, and their associations with incident CHD and stroke (composite outcome) were compared. A lower McAuley index and higher HOMA-IR are indicative of IR. Cox regression analysis was used to estimate adjusted hazard ratios for incident CHD and/or stroke. There were 158 events (89 CHD-only, 58 stroke-only, and 11 CHD/stroke) over a median follow-up of 8.4 years. After adjustment for demographic factors, the risk of the composite outcome decreased with each SD increase in the McAuley index (hazard ratio 0.80; 95% CI: 0.67-0.96), with no attenuation after further accounting for CHD and stroke risk factors. When considered individually, McAuley index and HOMA-IR were associated with CHD (hazard ratio 0.71, 95% CI: 0.55-0.92 and hazard ratio 1.33, 95% CI: 1.03-1.72, respectively), but not stroke risk. The logHOMA-IR and CHD association was present in men, but not in women (P=0.01).
Both HOMA-IR and the McAuley index demonstrate strong associations with CHD but not stroke risk in blacks. The logHOMA-IR and CHD association was present in men, but not in women.
探索黑人胰岛素抵抗(IR)与心血管疾病之间关联的研究尚无定论,尤其是对于冠心病(CHD)。麦考利指数和IR的稳态模型评估(HOMA-IR)在预测心血管疾病方面表现不同。我们在杰克逊心脏研究(一项针对黑人的大型纵向队列研究)中调查了这种关联。
在基线时,使用麦考利指数和HOMA-IR对3565名无糖尿病和心血管疾病的参与者进行IR评估,并比较它们与CHD和中风(复合结局)的关联。较低的麦考利指数和较高的HOMA-IR表明存在IR。使用Cox回归分析估计CHD和/或中风发病的调整后风险比。在中位随访8.4年期间,共发生158起事件(仅CHD 89起、仅中风58起、CHD/中风11起)。在调整人口统计学因素后,复合结局的风险随着麦考利指数每增加1个标准差而降低(风险比0.80;95%CI:0.67-0.96),在进一步考虑CHD和中风危险因素后无减弱。单独考虑时,麦考利指数和HOMA-IR与CHD相关(风险比分别为0.71,95%CI:0.55-0.92和风险比1.33,95%CI:1.03-1.72),但与中风风险无关。logHOMA-IR与CHD的关联在男性中存在,但在女性中不存在(P=0.01)。
HOMA-IR和麦考利指数均显示与黑人的CHD密切相关,但与中风风险无关。logHOMA-IR与CHD的关联在男性中存在,但在女性中不存在。