Department of Epidemiology and Preventive Medicine, School of Public Health, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel.
Leviev Heart Center, Sheba Medical Center, Ramat Gan, Israel.
Cardiovasc Diabetol. 2021 May 6;20(1):97. doi: 10.1186/s12933-021-01284-9.
Type 2 Diabetes is a major risk factor for cardiovascular (CV) mortality. Insulin resistance can be evaluated non-invasively by insulin sensitivity indices (ISI) such as the Mcauley index (MCAi), which is a function of the fasting insulin and triglycerides. Currently, the association between ISIs and ECG findings and all-cause and CV mortality is still not established in a large scale and heterogeneous population.
In a prospective study of the Israel cohort on Glucose Intolerance, Obesity and Hypertension (GOH) second phase (1979-1982) 1830 men and women were followed until December-2016 for CV-mortality and December-2019 for all-cause mortality. ECGs were recorded and OGTTs performed during baseline. ISIs were categorized into quartiles and evaluated against ECG findings and all-cause and CV-mortality.
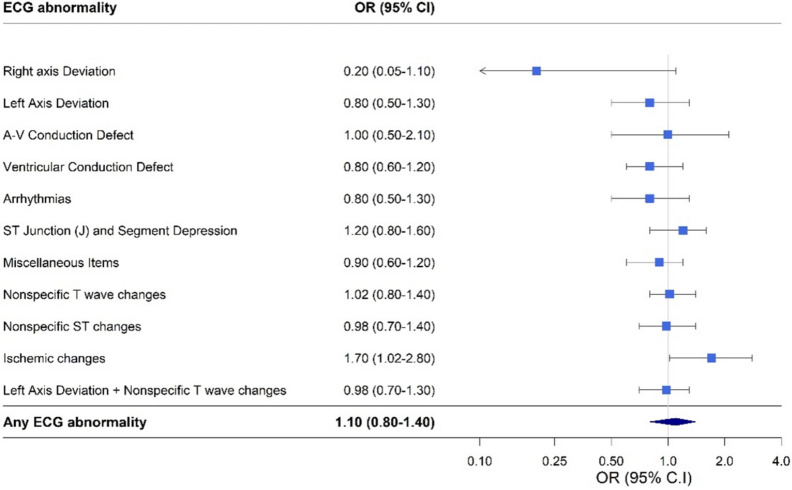
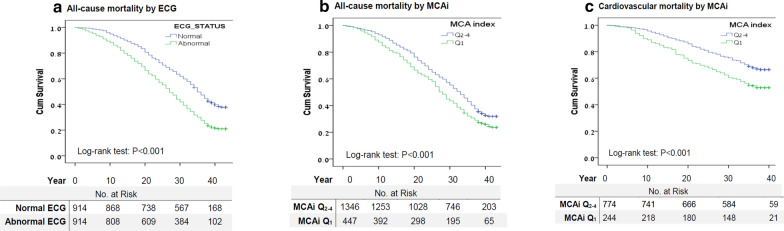
Mean age at baseline was 52.0 ± 8.1 years, and 75 (15.2%) and 47 (25.3%) participants in the upper quartiles (Q) and the lower quartile (Q) of the MCAi, presented with Ischemic changes on ECG respectively (p = 0.02). Multivariable analysis showed higher odds for ECG ischemic changes, for individuals in Q-MCAi (adjusted-OR = 1.7, 95% CI 1.02-2.8), compared with Q-MCAi, which attenuated when excluding individuals with diabetes (adjusted-OR = 1.6, 95% CI 0.9-2.7, p = 0.09). Median follow up for all-cause and for cardiovascular mortality was 31 years and 37 years, respectively. Cox proportional-hazards regression showed an increased risk for all-cause mortality for individuals in Q-MCAi (HR = 1.2, 95% CI 1.02-1.3) as well as an increased risk for CV-mortality (HR = 1.4, 95%CI 1.1-1.8) compared with Q-MCAi. Individuals in Q-Ln Homeostatic model assessment- Insulin Resistance (HOMA-IR) and Q- Quantitative Insulin Sensitivity Check Index (QUICKI) also presented with increased risk for all-cause-mortality (HR = 1.2, 95%CI 1.04-1.4; and HR = 1.2, 95% CI 1.04-1.4, respectively). Other ISIs did not show significant associations with CV-mortality.
Higher insulin-resistance, according to the MCAi, associated with ECG-changes, and with greater risk for all-cause and CV-mortality over a 40-year follow-up. The MCAi may be considered as an early predictive and prognostic biomarker for CV-morbidity and mortality in adults.
2 型糖尿病是心血管(CV)死亡率的主要危险因素。胰岛素抵抗可以通过胰岛素敏感性指数(ISI)进行非侵入性评估,如 Mcauley 指数(MCAi),它是空腹胰岛素和甘油三酯的函数。目前,在大规模和异质人群中,ISI 与心电图结果以及全因和心血管死亡率之间的关联尚未确定。
在以色列葡萄糖耐量、肥胖和高血压(GOH)第二阶段(1979-1982 年)的前瞻性研究中,1830 名男性和女性被随访至 2016 年 12 月(CV 死亡率)和 2019 年 12 月(全因死亡率)。在基线时记录心电图并进行 OGTT。将 ISI 分为四分位,并评估其与心电图结果以及全因和心血管死亡率的关系。
基线时的平均年龄为 52.0±8.1 岁,MCAi 上四分位数(Q)和下四分位数(Q)的 75 名(15.2%)和 47 名(25.3%)参与者的心电图存在缺血性改变(p=0.02)。多变量分析显示,与 Q-MCAi 相比,Q-MCAi 个体发生心电图缺血性改变的可能性更高(调整后 OR=1.7,95%CI 1.02-2.8),但排除糖尿病患者后减弱(调整后 OR=1.6,95%CI 0.9-2.7,p=0.09)。全因死亡率和心血管死亡率的中位随访时间分别为 31 年和 37 年。Cox 比例风险回归显示,与 Q-MCAi 相比,Q-MCAi 个体的全因死亡率风险增加(HR=1.2,95%CI 1.02-1.3),CV 死亡率风险也增加(HR=1.4,95%CI 1.1-1.8)。Q-Ln 稳态模型评估-胰岛素抵抗(HOMA-IR)和 Q-定量胰岛素敏感性检查指数(QUICKI)的个体也存在全因死亡率风险增加(HR=1.2,95%CI 1.04-1.4;和 HR=1.2,95%CI 1.04-1.4,分别)。其他 ISI 与 CV 死亡率无显著相关性。
根据 MCAi,较高的胰岛素抵抗与心电图变化相关,并与 40 年随访期间的全因和心血管死亡率风险增加相关。MCAi 可作为成人心血管发病率和死亡率的早期预测和预后生物标志物。