Kim Inna, Kim Min Chul, Jeong Hae Chang, Park Keun Ho, Sim Doo Sun, Hong Young Joon, Kim Ju Han, Jeong Myung Ho, Cho Jeong Gwan, Park Jong Chun, Seung Ki-Bae, Chang Kiyuk, Ahn Youngkeun
Department of Cardiology, Cardiovascular Center, Chonnam National University Hospital, Gwangju, Korea.
Department of Cardiology, Cardiovascular Center, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea.
Korean Circ J. 2017 Jan;47(1):36-43. doi: 10.4070/kcj.2015.0358. Epub 2016 Dec 12.
In patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease (MVD), the optimal timing of staged percutaneous coronary intervention (PCI) remains unclear.
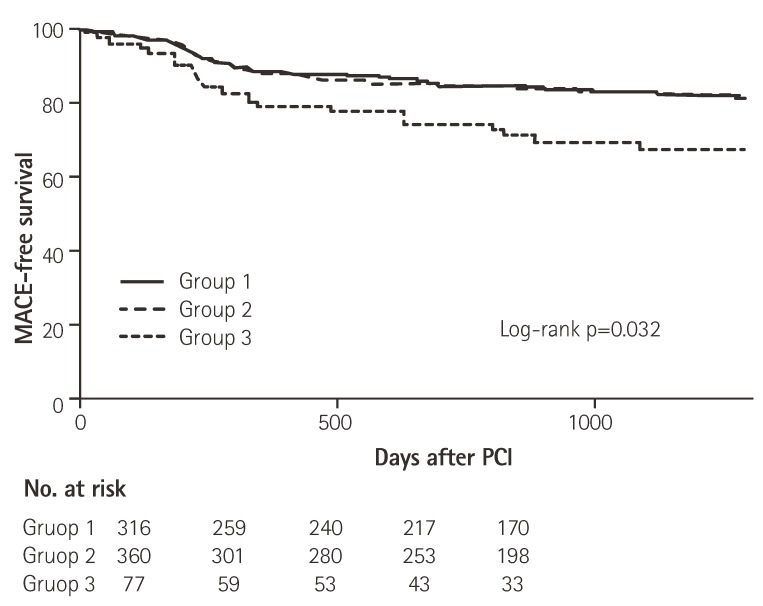
This study was a retrospective analysis of 753 STEMI patients with MVD who were treated by multivessel PCI in the Convergent Registry of Catholic and Chonnam University for Acute myocardial infarction (MI). Patients were divided into 3 groups according to the time from initial to staged PCI: group 1 (n=316, multivessel PCI performed during the index procedure), group 2 (n=360, staged PCI within 1 week), and group 3 (n=77, staged PCI after 1 week). The endpoint was major adverse cardiac events (MACEs), including all-cause mortality, non-fatal MI, and repeat PCI during 3.4 years follow-up.
The incidence of composite MACEs was higher in group 3 than in group 1 (odds ratio [OR]: 1.83, 95% confidence interval [CI]: 1.06 to 3.18, p=0.031). However, the risk of MACEs in groups 1 and 2 was comparable (OR: 1.01, 95% CI: 0.70 to 1.46, p=0.950). In multivariate logistic regression, independent predictors of 3-year MACEs were high Killip class (OR: 2.72, 95% CI: 1.38 to 5.37, p=0.004), left ventricular ejection fraction <45% (OR: 1.57, 95% CI: 1.06 to 2.32, p=0.024), and group 3 (OR: 1.83, 95% CI: 1.06 to 3.18, p=0.009).
Deferred staged PCI after one week index PCI was associated with the highest MACE, as compared to both simultaneous multivessel PCI and early staged PCI <1 week.
在ST段抬高型心肌梗死(STEMI)合并多支血管病变(MVD)的患者中,分期经皮冠状动脉介入治疗(PCI)的最佳时机仍不明确。
本研究是对天主教大学和全南大学急性心肌梗死(MI)汇聚登记处753例接受多支血管PCI治疗的STEMI合并MVD患者进行的回顾性分析。根据首次PCI至分期PCI的时间将患者分为3组:第1组(n = 316,在首次手术期间进行多支血管PCI),第2组(n = 360,在1周内进行分期PCI),第3组(n = 77,在1周后进行分期PCI)。终点为主要不良心脏事件(MACE),包括全因死亡率、非致命性MI以及3.4年随访期间的再次PCI。
第3组复合MACE的发生率高于第1组(优势比[OR]:1.83,95%置信区间[CI]:1.06至3.18,p = 0.031)。然而,第1组和第2组MACE的风险相当(OR:1.01,95% CI:0.70至1.46,p = 0.950)。在多因素逻辑回归中,3年MACE的独立预测因素为高Killip分级(OR:2.72