Wang Kyle, Mullins Brandon T, Falchook Aaron D, Lian Jun, He Kelei, Shen Dinggang, Dance Michael, Lin Weili, Sills Tiffany M, Das Shiva K, Huang Benjamin Y, Chera Bhishamjit S
Department of Radiation Oncology, University of North Carolina Hospitals , Chapel Hill, NC , USA.
State Key Laboratory for Novel Software Technology, Nanjing University , Nanjing , China.
Front Oncol. 2017 Jan 23;7:8. doi: 10.3389/fonc.2017.00008. eCollection 2017.
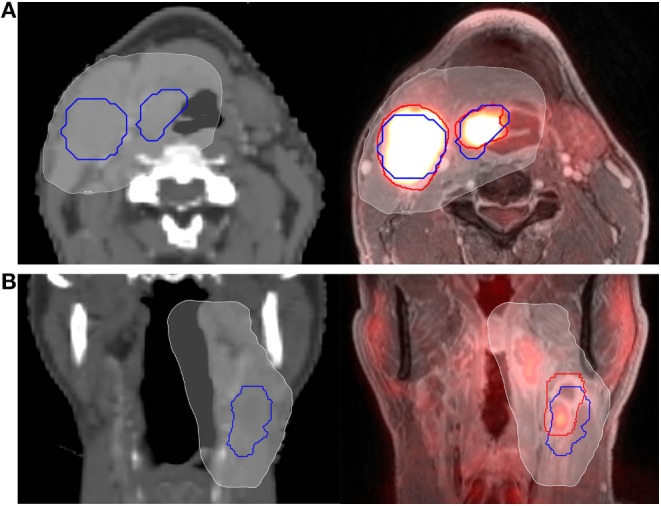
Computed tomography (CT), combined positron emitted tomography and CT (PET/CT), and magnetic resonance imaging (MRI) are commonly used in head and neck radiation planning. Hybrid PET/MRI has garnered attention for potential added value in cancer staging and treatment planning. Herein, we compare PET/MRI vs. planning CT for head and neck cancer gross tumor volume (GTV) delineation.
We prospectively enrolled patients with head and neck cancer treated with definitive chemoradiation to 60-70 Gy using IMRT. We performed pretreatment contrast-enhanced planning CT and gadolinium-enhanced PET/MRI. Primary and nodal volumes were delineated on planning CT (GTV-CT) prospectively before treatment and PET/MRI (GTV-PET/MRI) retrospectively after treatment. GTV-PET/MRI was compared to GTV-CT using separate rigid registrations for each tumor volume. The Dice similarity coefficient (DSC) metric evaluating spatial overlap and modified Hausdorff distance (mHD) evaluating mean orthogonal distance difference were calculated. Minimum dose to 95% of GTVs (D95) was compared.
Eleven patients were evaluable (10 oropharynx, 1 larynx). Nine patients had evaluable primary tumor GTVs and seven patients had evaluable nodal GTVs. Mean primary GTV-CT and GTV-PET/MRI size were 13.2 and 14.3 cc, with mean intersection 8.7 cc, DSC 0.63, and mHD 1.6 mm. D95 was 65.3 Gy for primary GTV-CT vs. 65.2 Gy for primary GTV-PET/MRI. Mean nodal GTV-CT and GTV-PET/MRI size were 19.0 and 23.0 cc, with mean intersection 14.4 cc, DSC 0.69, and mHD 2.3 mm. D95 was 62.3 Gy for both nodal GTV-CT and GTV-PET/MRI.
In this series of patients with head and neck (primarily oropharynx) cancer, PET/MRI and CT-GTVs had similar volumes (though there were individual cases with larger differences) with overall small discrepancies in spatial overlap, small mean orthogonal distance differences, and similar radiation doses.
计算机断层扫描(CT)、正电子发射断层扫描与CT联合(PET/CT)以及磁共振成像(MRI)常用于头颈部放射治疗计划。混合PET/MRI在癌症分期和治疗计划中的潜在附加价值已受到关注。在此,我们比较PET/MRI与计划CT对头颈部癌大体肿瘤体积(GTV)的勾画。
我们前瞻性纳入接受调强放疗(IMRT)、确定性放化疗、剂量为60 - 70 Gy的头颈部癌患者。我们在治疗前进行了增强对比计划CT和钆增强PET/MRI检查。在治疗前前瞻性地在计划CT(GTV-CT)上勾画原发灶和淋巴结体积,在治疗后回顾性地在PET/MRI(GTV-PET/MRI)上勾画。对每个肿瘤体积使用单独的刚性配准将GTV-PET/MRI与GTV-CT进行比较。计算评估空间重叠的Dice相似系数(DSC)指标和评估平均正交距离差异的改良豪斯多夫距离(mHD)。比较GTVs的95%所接受的最小剂量(D95)。
11例患者可评估(10例口咽癌,1例喉癌)。9例患者有可评估的原发肿瘤GTV,7例患者有可评估的淋巴结GTV。原发灶GTV-CT和GTV-PET/MRI的平均大小分别为13.2 cc和14.3 cc,平均交集为8.7 cc,DSC为0.63,mHD为1.6 mm。原发灶GTV-CT的D95为65.3 Gy,原发灶GTV-PET/MRI的D95为65.2 Gy。淋巴结GTV-CT和GTV-PET/MRI的平均大小分别为19.0 cc和23.0 cc,平均交集为14.4 cc,DSC为0.69,mHD为2.3 mm。淋巴结GTV-CT和GTV-PET/MRI的D95均为62.3 Gy。
在这组头颈部(主要是口咽)癌患者中,PET/MRI和CT-GTV的体积相似(尽管个别病例差异较大),总体空间重叠差异小,平均正交距离差异小,辐射剂量相似。