Reintam Blaser Annika, Starkopf Joel, Alhazzani Waleed, Berger Mette M, Casaer Michael P, Deane Adam M, Fruhwald Sonja, Hiesmayr Michael, Ichai Carole, Jakob Stephan M, Loudet Cecilia I, Malbrain Manu L N G, Montejo González Juan C, Paugam-Burtz Catherine, Poeze Martijn, Preiser Jean-Charles, Singer Pierre, van Zanten Arthur R H, De Waele Jan, Wendon Julia, Wernerman Jan, Whitehouse Tony, Wilmer Alexander, Oudemans-van Straaten Heleen M
Department of Anaesthesiology and Intensive Care, University of Tartu, Tartu, Estonia.
Center of Intensive Care Medicine, Lucerne Cantonal Hospital, Lucerne, Switzerland.
Intensive Care Med. 2017 Mar;43(3):380-398. doi: 10.1007/s00134-016-4665-0. Epub 2017 Feb 6.
To provide evidence-based guidelines for early enteral nutrition (EEN) during critical illness.
We aimed to compare EEN vs. early parenteral nutrition (PN) and vs. delayed EN. We defined "early" EN as EN started within 48 h independent of type or amount. We listed, a priori, conditions in which EN is often delayed, and performed systematic reviews in 24 such subtopics. If sufficient evidence was available, we performed meta-analyses; if not, we qualitatively summarized the evidence and based our recommendations on expert opinion. We used the GRADE approach for guideline development. The final recommendations were compiled via Delphi rounds.
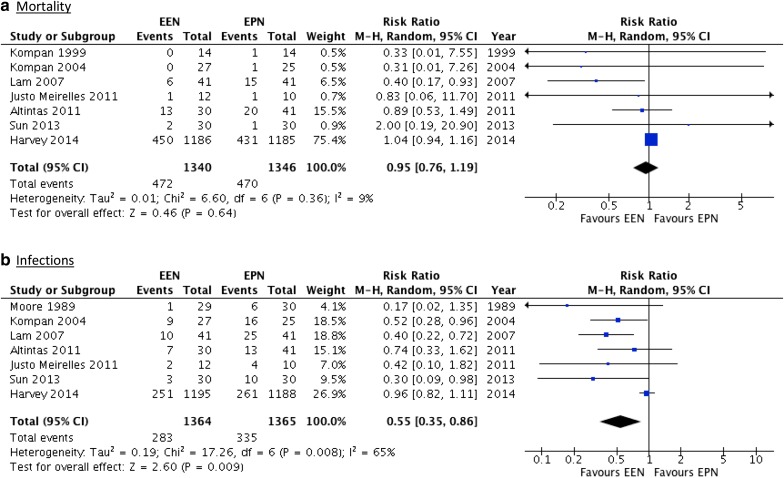
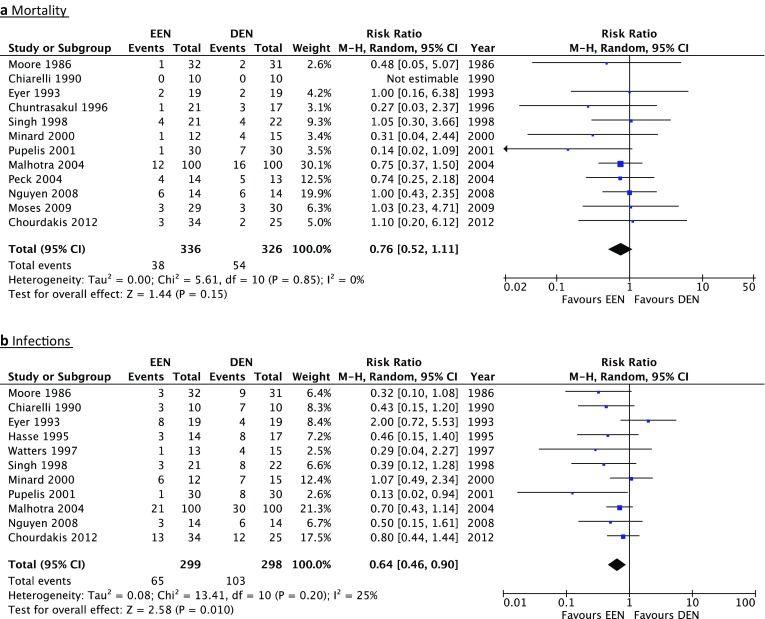
We formulated 17 recommendations favouring initiation of EEN and seven recommendations favouring delaying EN. We performed five meta-analyses: in unselected critically ill patients, and specifically in traumatic brain injury, severe acute pancreatitis, gastrointestinal (GI) surgery and abdominal trauma. EEN reduced infectious complications in unselected critically ill patients, in patients with severe acute pancreatitis, and after GI surgery. We did not detect any evidence of superiority for early PN or delayed EN over EEN. All recommendations are weak because of the low quality of evidence, with several based only on expert opinion.
We suggest using EEN in the majority of critically ill under certain precautions. In the absence of evidence, we suggest delaying EN in critically ill patients with uncontrolled shock, uncontrolled hypoxaemia and acidosis, uncontrolled upper GI bleeding, gastric aspirate >500 ml/6 h, bowel ischaemia, bowel obstruction, abdominal compartment syndrome, and high-output fistula without distal feeding access.
为危重症期间的早期肠内营养(EEN)提供循证指南。
我们旨在比较EEN与早期肠外营养(PN)以及延迟肠内营养。我们将“早期”肠内营养定义为在48小时内开始的肠内营养,与类型或数量无关。我们预先列出了肠内营养经常延迟的情况,并对24个此类子主题进行了系统评价。如果有足够的证据,我们进行荟萃分析;如果没有,我们定性总结证据并根据专家意见提出建议。我们使用GRADE方法制定指南。最终建议通过德尔菲轮次汇总而成。
我们制定了17条支持启动EEN的建议和7条支持延迟肠内营养的建议。我们进行了五项荟萃分析:在未选择的危重症患者中,特别是在创伤性脑损伤、重症急性胰腺炎、胃肠道(GI)手术和腹部创伤患者中。EEN降低了未选择的危重症患者、重症急性胰腺炎患者和胃肠道手术后患者的感染并发症。我们没有发现早期PN或延迟肠内营养优于EEN的证据。由于证据质量低,所有建议的力度都较弱,其中几条仅基于专家意见。
我们建议在采取某些预防措施的情况下,对大多数危重症患者使用EEN。在缺乏证据的情况下,我们建议对休克未控制、低氧血症和酸中毒未控制、上消化道出血未控制、胃吸出物>500 ml/6小时、肠缺血、肠梗阻、腹腔间隔室综合征以及无远端喂养通路的高流量瘘的危重症患者延迟肠内营养。