Girum Tadele, Kote Mesfin, Tariku Befikadu, Bekele Henok
Department of Public Health, College of Medicine and Health Sciences, Wolkite University, Wolkite.
Department of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch.
Ther Clin Risk Manag. 2017 Jan 23;13:101-110. doi: 10.2147/TCRM.S119826. eCollection 2017.
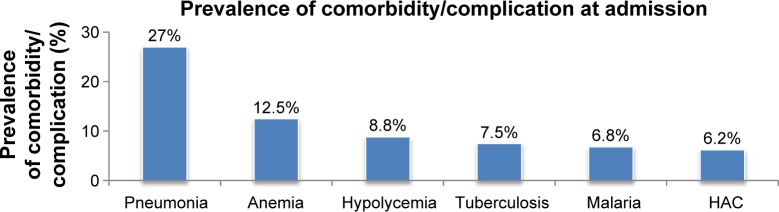
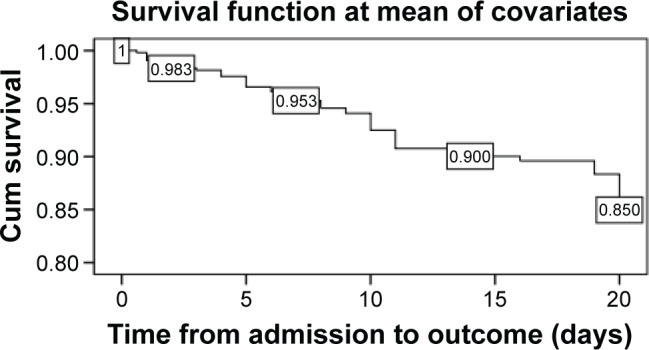
Despite the existence of standard protocol, many stabilization centers (SCs) continue to experience high mortality of children receiving treatment for severe acute malnutrition. Assessing treatment outcomes and identifying predictors may help to overcome this problem. Therefore, a 30-month retrospective cohort study was conducted among 545 randomly selected medical records of children <5 years of age admitted to SCs in Gedeo Zone. Data was entered by Epi Info version 7 and analyzed by STATA version 11. Cox proportional hazards model was built by forward stepwise procedure and compared by the likelihood ratio test and Harrell's concordance, and fitness was checked by Cox-Snell residual plot. During follow-up, 51 (9.3%) children had died, and 414 (76%) and 26 (4.8%) children had recovered and defaulted (missed follow-up for 2 consecutive days), respectively. The survival rates at the end of the first, second and third weeks were 95.3%, 90% and 85%, respectively, and the overall mean survival time was 79.6 days. Age <24 months (adjusted hazard ratio [AHR] =2.841, 95% confidence interval [CI] =1.101-7.329), altered pulse rate (AHR =3.926, 95% CI =1.579-9.763), altered temperature (AHR =7.173, 95% CI =3.05-16.867), shock (AHR =3.805, 95% CI =1.829-7.919), anemia (AHR =2.618, 95% CI =1.148-5.97), nasogastric tube feeding (AHR =3.181, 95% CI =1.18-8.575), hypoglycemia (AHR =2.74, 95% CI =1.279-5.87) and treatment at hospital stabilization center (AHR =4.772, 95% CI =1.638-13.9) were independent predictors of mortality. The treatment outcomes and incidence of death were in the acceptable ranges of national and international standards. Intervention to further reduce deaths has to focus on young children with comorbidities and altered general conditions.
尽管存在标准治疗方案,但许多营养稳定中心(SCs)在为重度急性营养不良儿童提供治疗时,儿童死亡率仍然很高。评估治疗结果并确定预测因素可能有助于解决这一问题。因此,我们对随机抽取的545份盖德奥地区营养稳定中心收治的5岁以下儿童的病历进行了一项为期30个月的回顾性队列研究。数据通过Epi Info 7版本录入,并使用STATA 11版本进行分析。通过向前逐步法构建Cox比例风险模型,并通过似然比检验和Harrell一致性进行比较,通过Cox-Snell残差图检查模型拟合度。在随访期间,51名(9.3%)儿童死亡,414名(76%)儿童康复,26名(4.8%)儿童失访(连续2天未进行随访)。第一周、第二周和第三周结束时的生存率分别为95.3%、90%和85%,总体平均生存时间为79.6天。年龄小于24个月(调整后风险比[AHR]=2.841,95%置信区间[CI]=1.101-7.329)、脉搏率改变(AHR=3.926,95%CI=1.579-9.763)、体温改变(AHR=7.173,95%CI=3.05-16.867)、休克(AHR=3.805,95%CI=1.829-7.919)、贫血(AHR=2.618,95%CI=1.148-5.97)、鼻胃管喂养(AHR=3.181,95%CI=1.18-8.575)、低血糖(AHR=2.74,95%CI=1.279-5.87)以及在医院营养稳定中心接受治疗(AHR=4.772,95%CI=1.638-13.9)是死亡的独立预测因素。治疗结果和死亡率在国家和国际标准的可接受范围内。进一步降低死亡的干预措施必须侧重于患有合并症和一般状况改变的幼儿。