Lönnberg Stefan, Andreassen Trude, Engesæter Birgit, Lilleng Rune, Kleven Cecilia, Skare Annelie, Johansson Karin, Fredheim Christina Stangeland, Tropé Ameli
Cancer Registry of Norway, Oslo, Norway.
Department of Pathology, Vestre Viken Hospital Trust, Drammen, Norway.
BMJ Open. 2016 Nov 14;6(11):e013728. doi: 10.1136/bmjopen-2016-013728.
The main barrier to optimal effect in many established population-based screening programmes against cervical cancer is low participation. In Norway, a routine health service integrated population-based screening programme has been running since 1995, using open invitations and reminders. The aim of this randomised health service study was to pilot scheduled appointments and assess their potential for increased participation.
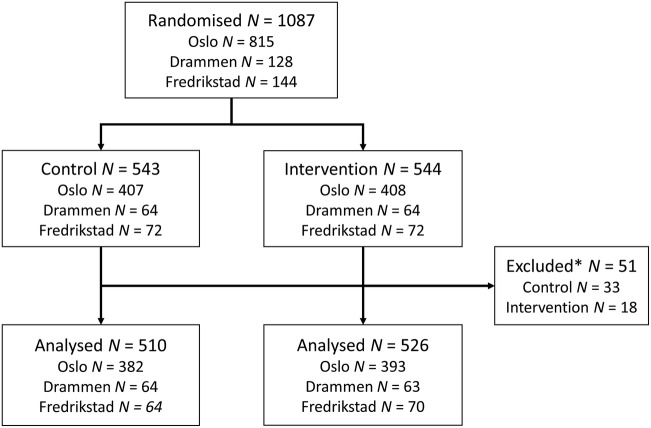
Within the national screening programme, we randomised 1087 women overdue for screening to receive invitations with scheduled appointments (intervention) or the standard open reminders (control). Letters were sent 2-4 weeks before the scheduled appointments at three centres: a midwife clinic, a public healthcare centre and a general practitioner centre. The primary outcome was participation at 6 months of follow-up. Secondary outcomes were participation at 1 and 3 months. Risk ratios (RRs) overall, and stratified by screening centre, age group and previous participation, were calculated using log-binomial regression.
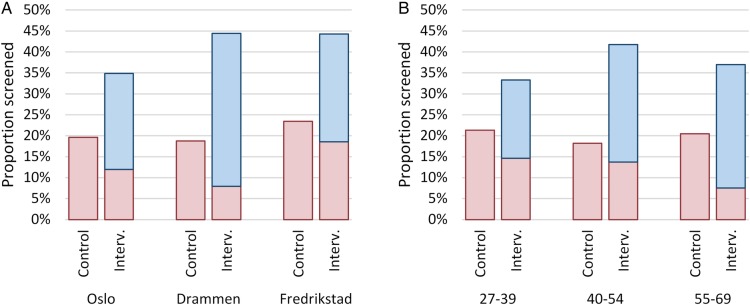
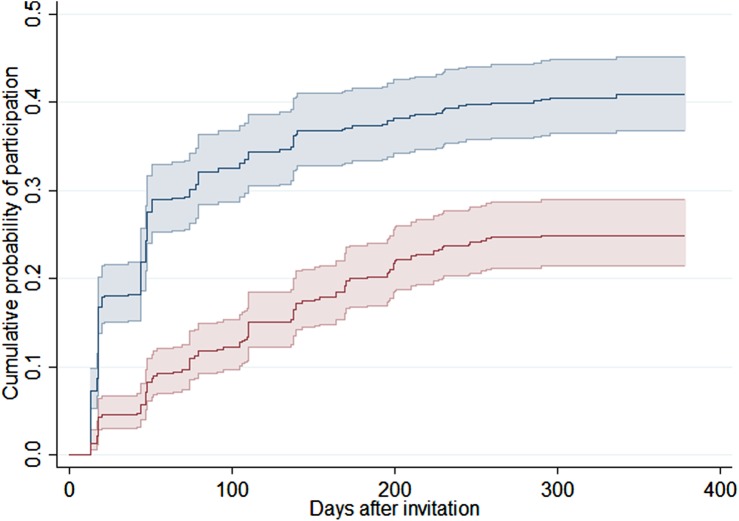
At 6 months, 20% of the 510 women in the control group and 37% of the 526 women in the intervention group had participated in screening, excluding 51 women in total from analysis due to participation just before invitation and therefore not yet visible in the central records. The RR for participation at 6 months was 1.9 (95% CI 1.5 to 2.3). There was no significant heterogeneity between centres or age groups. Participation increased among women both with (RR 1.7; 95% CI 1.4 to 2.1) and without (RR 3.5; 95% CI 1.3 to 9.2) previous participation. The RRs for participation at 1 and 3 months were 4.0 (95% CI 2.6 to 6.2) and 2.7 (95% CI 2.1 to 3.5), respectively.
Scheduled appointments increased screening participation consistently across all target ages and screening centres among women overdue for screening. Participation increased also among women with no previous records of cervical screening.
在许多已确立的基于人群的宫颈癌筛查项目中,实现最佳效果的主要障碍是参与率低。在挪威,自1995年以来一直在实施一项常规卫生服务综合人群筛查项目,采用公开邀请和提醒的方式。这项随机卫生服务研究的目的是试行预约安排并评估其提高参与率的潜力。
在国家筛查项目中,我们将1087名逾期未筛查的女性随机分为两组,一组接受预约邀请(干预组),另一组接受标准的公开提醒(对照组)。在三个中心(一家助产士诊所、一家公共医疗中心和一家全科医生中心)于预约前2至4周发送信件。主要结局是随访6个月时的参与情况。次要结局是随访1个月和3个月时的参与情况。使用对数二项回归计算总体及按筛查中心、年龄组和既往参与情况分层的风险比(RR)。
6个月时,对照组510名女性中有20%参与了筛查,干预组526名女性中有37%参与了筛查,共有51名女性因在邀请前刚刚参与筛查而未纳入分析,因为她们在中心记录中尚未显示。6个月时参与筛查的RR为1.9(95%CI 1.5至2.3)。各中心或年龄组之间无显著异质性。既往参与过筛查的女性(RR 1.7;95%CI 1.4至2.1)和未参与过筛查的女性(RR 3.5;95%CI 1.3至9.2)的参与率均有所提高。1个月和3个月时参与筛查的RR分别为4.0(95%CI 2.6至6.2)和2.7(95%CI 2.1至3.5)。
预约安排使逾期未筛查女性在所有目标年龄组和筛查中心的筛查参与率均持续提高。既往无宫颈癌筛查记录的女性的参与率也有所提高。