Elshobary Mohamed, Shehta Ahmed, Salah Tarek, Sultan Ahmed Mohamed, Shiha Usama, Elghawalby Ahmed Nabieh, Monier Ahmed, Elsadany Mohamed, Fathy Omar, Wahab Mohamed Abdel
Liver Transplantation Unit, Gatroenterology Surgical Centre, College of Medicine, Mansoura University, Egypt.
Liver Transplantation Unit, Gatroenterology Surgical Centre, College of Medicine, Mansoura University, Egypt.
Int J Surg Case Rep. 2017;31:214-217. doi: 10.1016/j.ijscr.2016.12.020. Epub 2017 Jan 5.
In adult living donor liver transplantation (LDLT), maintenance of adequate portal inflow is essential for the graft regeneration. Portal inflow steal (PFS) may occur due to presence of huge spontaneous porto-systemic collaterals. A surgical procedure to increase the portal inflow is rarely necessary in adult LDLT.
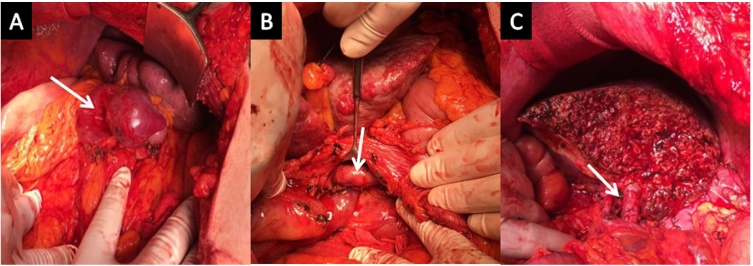
A 52 years male patient with end-stage liver disease due to chronic hepatitis C virus infection. Preoperative portography showed marked attenuated portal vein and its two main branches, patent tortuous splenic vein, multiple splenic hilar collaterals, and large lieno-renal collateral. He received a right hemi-liver graft from his nephew. Exploration revealed markedly cirrhotic liver, moderate splenomegaly with multiple collaterals and large lieno-renal collateral. Upon dissection of the hepato-duodenal ligament, a well-developed portal vein could be identified with a small mural thrombus. The recipient portal vein stump was anastomosed, in end to end fashion, to the graft portal vein. Doppler US showed reduced portal vein flow, so ligation of the huge lieno-renal collateral that allows steal of the portal inflow. After ligation of the lieno-renal collateral, improvement of the portal vein flow was observed in Doppler US.
There is no accepted algorithm for managing spontaneous lieno-renal shunts before, during, or after liver transplantation, and evidence for efficacy of treatments remains limited. We report a case of surgical interruption of spontaneous huge porto-systemic collateral to prevent PFS during adult LDLT.
Complete interruption of large collateral vessels might be needed as a part of adult LDLT procedure to avoid devastating postoperative PFS.
在成人活体肝移植(LDLT)中,维持充足的门静脉血流对移植物再生至关重要。由于存在巨大的自发性门体侧支循环,可能会发生门静脉血流窃流(PFS)。在成人LDLT中,很少需要通过手术来增加门静脉血流。
一名52岁男性患者,因慢性丙型肝炎病毒感染导致终末期肝病。术前门静脉造影显示门静脉及其两个主要分支明显变细,脾静脉迂曲且通畅,脾门处有多个侧支循环,以及巨大的脾肾侧支循环。他接受了来自其侄子的右半肝移植。术中探查发现肝脏明显肝硬化,脾脏中度肿大,有多个侧支循环和巨大的脾肾侧支循环。在解剖肝十二指肠韧带时,可识别出一条发育良好的门静脉,伴有一小片壁内血栓。将受体门静脉残端与移植物门静脉进行端端吻合。多普勒超声显示门静脉血流减少,因此结扎了导致门静脉血流窃流的巨大脾肾侧支循环。结扎脾肾侧支循环后,多普勒超声显示门静脉血流有所改善。
对于肝移植术前、术中和术后自发性脾肾分流的处理,目前尚无公认的方案,且治疗效果的证据仍然有限。我们报告了一例在成人LDLT期间通过手术中断自发性巨大门体侧支循环以预防PFS的病例。
作为成人LDLT手术的一部分,可能需要完全中断大的侧支血管,以避免术后发生严重的PFS。