Tsang Mazie, Parikh Sameer A
Division of Hematology, Department of Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Curr Hematol Malig Rep. 2017 Feb;12(1):29-38. doi: 10.1007/s11899-017-0366-1.
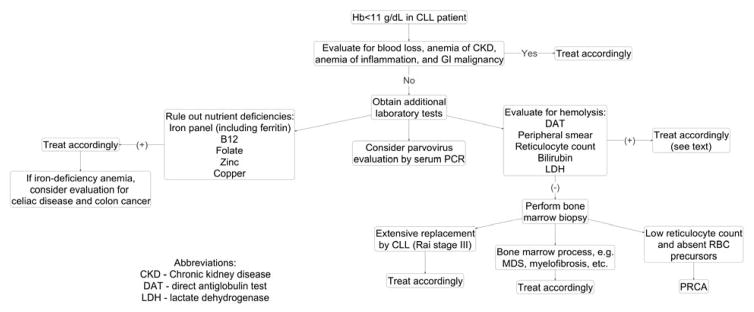
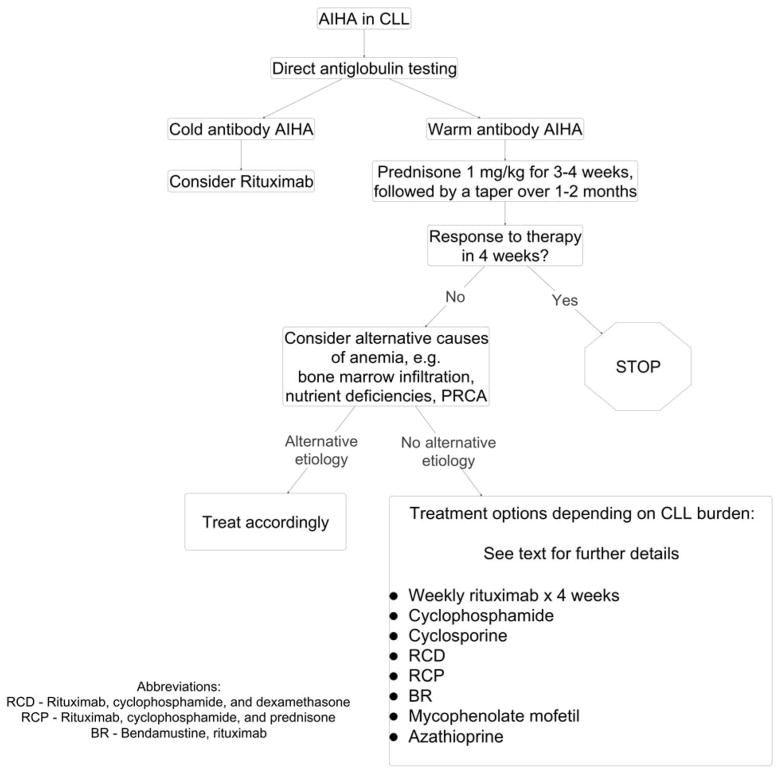
Chronic lymphocytic leukemia (CLL) is frequently associated with autoimmune complications such as autoimmune hemolytic anemia, immune thrombocytopenia, pure red cell aplasia, and autoimmune granulocytopenia. It is critical to diagnose cytopenias from these secondary complications of CLL accurately, since prognosis and therapy are substantially different from patients who have cytopenias due to extensive bone marrow infiltration by CLL. The pathogenesis of autoimmune cytopenias in CLL is complex; and it involves antigen presentation by CLL cells to polyclonal B cells resulting in production of autoantibody, and alteration of the T cell milieu tilting the balance in favor of an autoimmune response. Traditional therapy of autoimmune complications in CLL consists of immunosuppression with corticosteroids and/or anti-CD20 monoclonal antibodies. In patients who have a suboptimal response, treating the underlying CLL is generally effective in ameliorating secondary cytopenias. Although novel oral therapies such as ibrutinib, idelalisib, and venetoclax have been shown to be extremely effective in the management of CLL, prospective data from larger numbers of patients with longer follow-up are needed prior to recommending their routine use in the management of autoimmune cytopenias in CLL.
慢性淋巴细胞白血病(CLL)常伴有自身免疫性并发症,如自身免疫性溶血性贫血、免疫性血小板减少症、纯红细胞再生障碍性贫血和自身免疫性粒细胞减少症。准确诊断CLL这些继发性并发症导致的血细胞减少至关重要,因为其预后和治疗与因CLL广泛骨髓浸润导致血细胞减少的患者有很大不同。CLL中自身免疫性血细胞减少的发病机制复杂,涉及CLL细胞向多克隆B细胞呈递抗原导致自身抗体产生,以及T细胞环境改变使平衡倾向于自身免疫反应。CLL自身免疫性并发症的传统治疗包括使用皮质类固醇和/或抗CD20单克隆抗体进行免疫抑制。对于反应欠佳的患者,治疗潜在的CLL通常对改善继发性血细胞减少有效。尽管新型口服疗法如伊布替尼、idelalisib和维奈托克已被证明在CLL管理中极其有效,但在推荐其常规用于CLL自身免疫性血细胞减少的管理之前,需要来自更多患者、更长随访时间的前瞻性数据。