Davies Bethan, Turner Katy M E, Leung Stella, Yu B Nancy, Frølund Maria, Benfield Thomas, Blanchard James, Westh Henrik, Ward Helen
Department of Infectious Disease Epidemiology, School of Public Health, Imperial College London, London, United Kingdom.
School of Veterinary Science, University of Bristol, Langford, Bristol, United Kingdom.
PLoS One. 2017 Feb 15;12(2):e0171551. doi: 10.1371/journal.pone.0171551. eCollection 2017.
The impact of Chlamydia trachomatis (chlamydia) control on the incidence of pelvic inflammatory disease (PID) is theoretically limited by the proportion of PID caused by chlamydia. We estimate the population excess fraction (PEF) of treated chlamydia infection on PID at 12-months in settings with widespread chlamydia control (testing and treatment) and compare this to the estimated PEF of untreated chlamydia.
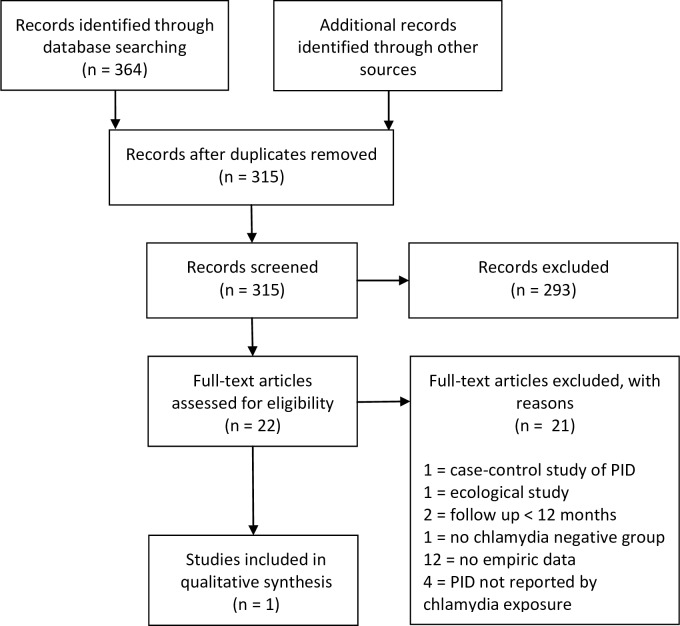
We used two large retrospective population-based cohorts of women of reproductive age from settings with widespread chlamydia control to calculate the PEF of treated chlamydia on PID at 12-months. We undertook a systematic review to identify further studies that reported the risk of PID in women who were tested for chlamydia (infected and uninfected). We used the same method to calculate the PEF in eligible studies then compared all estimates of PEF.
The systematic review identified a single study, a randomised controlled trial of chlamydia screening (POPI-RCT). In the presence of testing and treatment <10% of PID at 12-months was attributable to treated (baseline) chlamydia infections (Manitoba: 8.86%(95%CI 7.15-10.75); Denmark: 3.84%(3.26-4.45); screened-arm POPI-RCT: 0.99%(0.00-29.06)). In the absence of active chlamydia treatment 26.44%(11.57-46.32) of PID at 12-months was attributable to untreated (baseline) chlamydia infections (deferred-arm POPI-RCT). The PEFs suggest that eradicating baseline chlamydia infections could prevent 484 cases of PID at 12-months per 100,000 women in the untreated setting and 13-184 cases of PID per 100,000 tested women in the presence of testing and treatment.
Testing and treating chlamydia reduced the PEF of chlamydia on PID by 65% compared to the untreated setting. But in the presence of testing and treatment over 90% of PID could not be attributed to a baseline chlamydia infection. More information is needed about the aetiology of PID to develop effective strategies for improving the reproductive health of women.
沙眼衣原体(衣原体)感染防控措施对盆腔炎(PID)发病率的影响,理论上受衣原体所致PID占比的限制。我们估计在衣原体感染防控广泛开展(检测和治疗)的环境中,接受治疗的衣原体感染在12个月时对PID的人群超额分数(PEF),并将其与未治疗衣原体的估计PEF进行比较。
我们使用了两个基于人群的大型回顾性队列,研究对象为来自衣原体感染防控广泛开展地区的育龄女性,以计算接受治疗的衣原体感染在12个月时对PID的PEF。我们进行了一项系统评价,以确定更多报告衣原体检测(感染和未感染)女性PID风险的研究。我们使用相同方法计算符合条件研究中的PEF,然后比较所有PEF估计值。
系统评价仅识别出一项研究,即衣原体筛查的随机对照试验(POPI-RCT)。在有检测和治疗的情况下,12个月时<10%的PID可归因于接受治疗的(基线)衣原体感染(曼尼托巴:8.86%(95%CI 7.15 - 10.75);丹麦:3.84%(3.26 - 4.45);筛查组POPI-RCT:0.99%(0.00 - 29.06))。在没有积极衣原体治疗的情况下,12个月时26.44%(11.57 - 46.32)的PID可归因于未治疗的(基线)衣原体感染(延迟组POPI-RCT)。PEF表明,根除基线衣原体感染可在未治疗情况下每100,000名女性中预防12个月时484例PID,在有检测和治疗的情况下每100,000名接受检测的女性中预防13 - 184例PID。
与未治疗情况相比,检测和治疗衣原体使衣原体对PID的PEF降低了65%。但在有检测和治疗的情况下,超过90%的PID不能归因于基线衣原体感染。需要更多关于PID病因的信息,以制定改善女性生殖健康的有效策略。