Hirakawa Haruki, Nakashima Chiho, Nakamura Tomomi, Masuda Masanori, Funakoshi Taro, Nakagawa Shunsaku, Horimatsu Takahiro, Matsubara Kazuo, Muto Manabu, Kimura Shinya, Sueoka-Aragane Naoko
Division of Hematology, Respiratory Medicine and Oncology, Department of Internal Medicine, Faculty of Medicine, Naoko Sueoka-Aragane, Saga University, 5-1-1 Nabeshima, Saga, 849-8501, Japan.
Department of Pathology, Faculty of Medicine, Saga University Hospital, Saga, Japan.
J Med Case Rep. 2017 Feb 16;11(1):43. doi: 10.1186/s13256-017-1213-7.
The safety and efficacy of chemotherapy for patients undergoing concomitant hemodialysis have not been fully established and optimal doses of anti-cancer drugs and best timing of hemodialysis remains unclear. Although chemosensitive cancers, such as germ cell tumors, treated with chemotherapy should have sufficient dose intensity maintained to achieve the desired effect, many patients with cancer undergoing hemodialysis might be under-treated because the pharmacokinetics of anti-cancer drugs in such patients remains unknown.
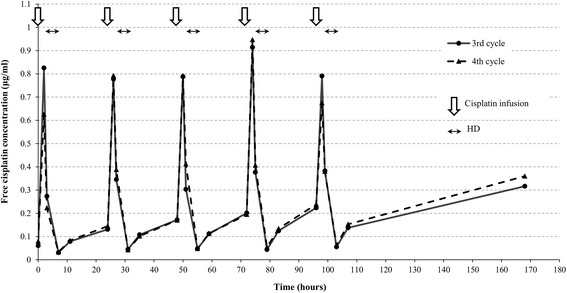
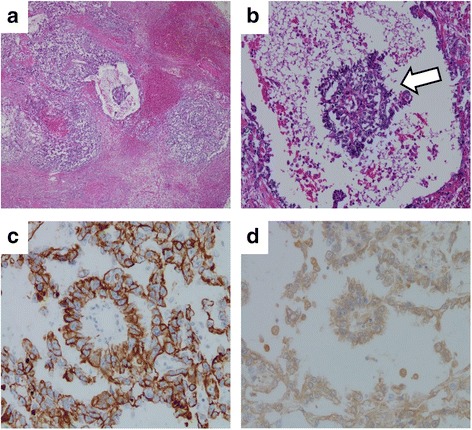
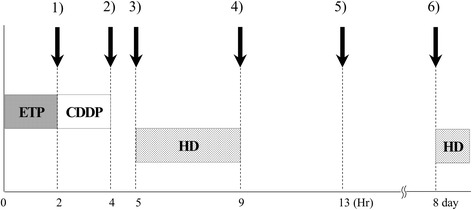
We describe a 31-year-old Japanese man with a mediastinal yolk sac tumor treated with surgery followed by five cycles of chemotherapy containing cisplatin and etoposide while concomitantly undergoing hemodialysis. The doses of these agents used in the first cycle were 50% of the standard dose of cisplatin (10 mg/m) and 60% of the standard dose of etoposide (60 mg/m) on days 1 through to 5; the doses were subsequently escalated to 75% with both agents. Hemodialysis was started 1 hour after infusions of these agents. Severe hematological toxicities were observed despite successful treatment. During treatment with concurrent hemodialysis, pharmacokinetic analysis of cisplatin was performed and its relationship with adverse effects was assessed. Compared with patients with normal renal function, the maximum drug concentration was higher, and concentration increased in the interval between hemodialysis and the subsequent cisplatin infusion, resulting in a higher area under the curve despite a reduction in the dose to 75% of the standard regimen.
Because of the altered pharmacokinetics pharmacodynamics status of patients with renal dysfunction undergoing hemodialysis, pharmacokinetics pharmacodynamics analysis is deemed to be helpful for effective and safe management of chemotherapy in patients undergoing hemodialysis.
对于同时进行血液透析的患者,化疗的安全性和有效性尚未完全确立,抗癌药物的最佳剂量和血液透析的最佳时机仍不明确。虽然对于化疗敏感的癌症,如生殖细胞肿瘤,应维持足够的剂量强度以达到预期效果,但许多接受血液透析的癌症患者可能未得到充分治疗,因为此类患者体内抗癌药物的药代动力学尚不清楚。
我们描述了一名31岁的日本男性,患有纵隔卵黄囊瘤,接受了手术治疗,随后在同时进行血液透析的情况下接受了五个周期含顺铂和依托泊苷的化疗。第一个周期中这些药物的剂量为顺铂标准剂量(10mg/m²)的50%和依托泊苷标准剂量(60mg/m²)的60%,于第1至5天使用;随后两种药物的剂量均增至75%。在输注这些药物1小时后开始血液透析。尽管治疗成功,但仍观察到严重的血液学毒性。在同时进行血液透析治疗期间,对顺铂进行了药代动力学分析,并评估了其与不良反应的关系。与肾功能正常的患者相比,最大药物浓度更高,且在血液透析与随后的顺铂输注之间的时间段内浓度升高,尽管剂量降至标准方案的75%,曲线下面积仍更高。
由于接受血液透析的肾功能不全患者的药代动力学和药效学状态发生改变,药代动力学和药效学分析被认为有助于对接受血液透析的患者进行有效且安全的化疗管理。