Pierce Brian, Bole Indra, Patel Vaiibhav, Brown David L
Hospitalist Division, Washington University School of Medicine, St. Louis, MO.
Cardiovascular Division, Washington University School of Medicine, St. Louis, MO
J Am Heart Assoc. 2017 Feb 20;6(2):e004666. doi: 10.1161/JAHA.116.004666.
Multiple randomized controlled trials of remote ischemic preconditioning (RIPC) prior to cardiac surgery have failed to demonstrate clinical benefit. The aim of this updated meta-analysis was to evaluate the effect of RIPC on outcomes following cardiac surgery.
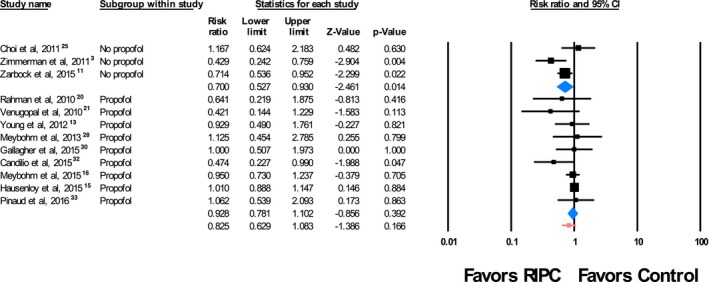
Searches of PubMed, Cochrane, EMBASE, and Web of Science databases were performed for 1970 to December 13, 2015. Randomized controlled trials comparing RIPC with a sham procedure prior to cardiac surgery performed with cardiopulmonary bypass were assessed. All-cause mortality, acute kidney injury (AKI), and myocardial infarction were the primary outcomes of interest. We identified 21 trials that randomized 5262 patients to RIPC or a sham procedure undergoing cardiac surgery. The majority of patients were men (72.6%) and the mean or median age ranged from 42.3 to 76.3 years. Of the 9 trials that evaluated mortality, 188 deaths occurred out of a total of 4210 randomized patients, with 96 deaths occurring in 2098 patients (4.6%) randomized to RIPC and 92 deaths occurring in 2112 patients (4.4%) randomized to a sham control procedure, demonstrating no significant reduction in all-cause mortality (risk ratio [RR], 0.987; 95% CI, 0.653-1.492, =0.95). Twelve studies evaluated AKI in 4209 randomized patients. In these studies, AKI was observed in 516 of 2091 patients (24.7%) undergoing RIPC and in 577 of 2118 patients (27.2%) randomized to a sham procedure. RIPC did not result in a significant reduction in AKI (RR, 0.839; 95% CI, 0.703-1.001 [=0.052]). In 6 studies consisting of 3799 randomized participants, myocardial infarction occurred in 237 of 1891 patients (12.5%) randomized to RIPC and in 282 of 1908 patients (14.8%) randomized to a sham procedure, resulting in no significant reduction in postoperative myocardial infarction (RR, 0.809; 95% CI, 0.615-1.064 [=0.13]). A subgroup analysis was performed a priori based on previous studies suggesting that propofol may mitigate the protective benefits of RIPC. Three studies randomized patients undergoing cardiac surgery to RIPC or sham procedure in the absence of propofol anesthesia. Most of these patients were men (60.3%) and the mean or median age ranged from 57.0 to 70.6 years. In this propofol-free subgroup of 434 randomized patients, 71 of 217 patients (32.7%) who underwent RIPC developed AKI compared with 103 of 217 patients (47.5%) treated with a sham procedure. In this cohort, RIPC resulted in a significant reduction in AKI (RR, 0.700; 95% CI, 0.527-0.930 [=0.014]). In studies of patients who received propofol anesthesia, 445 of 1874 (23.7%) patients randomized to RIPC developed AKI compared with 474 of 1901 (24.9%) who underwent a sham procedure. The RR for AKI was 0.928 (95% CI, 0.781-1.102; =0.39) for RIPC versus sham. There was no significant interaction between the two subgroups (=0.098).
RIPC does not reduce morbidity or mortality in patients undergoing cardiac surgery with cardiopulmonary bypass. In the subgroup of studies in which propofol was not used, a reduction in AKI was seen, suggesting that propofol may interact with the protective effects of RIPC. Future studies should evaluate RIPC in the absence of propofol anesthesia.

多项关于心脏手术前远程缺血预处理(RIPC)的随机对照试验未能证明其临床益处。这项更新的荟萃分析旨在评估RIPC对心脏手术后结局的影响。
检索了1970年至2015年12月13日的PubMed、Cochrane、EMBASE和科学网数据库。评估了在体外循环心脏手术前将RIPC与假手术进行比较的随机对照试验。全因死亡率、急性肾损伤(AKI)和心肌梗死是主要关注的结局。我们确定了21项试验,这些试验将5262例患者随机分为RIPC组或接受心脏手术的假手术组。大多数患者为男性(72.6%),平均或中位年龄在42.3至76.3岁之间。在评估死亡率的9项试验中,4210例随机分组患者中共有188例死亡,其中2098例随机分配至RIPC组的患者中有96例死亡(4.6%),2112例随机分配至假对照手术组的患者中有92例死亡(4.4%),表明全因死亡率无显著降低(风险比[RR],0.987;95%置信区间,0.653 - 1.492,P = 0.95)。12项研究评估了4209例随机分组患者的AKI情况。在这些研究中,接受RIPC的2091例患者中有516例(24.7%)发生AKI,随机分配至假手术组的2118例患者中有577例(27.2%)发生AKI。RIPC并未使AKI显著降低(RR,0.839;95%置信区间,0.703 - 1.001 [P = 0.052])。在由3799例随机参与者组成的6项研究中,随机分配至RIPC组的1891例患者中有237例(12.5%)发生心肌梗死,随机分配至假手术组 的1908例患者中有282例(14.8%)发生心肌梗死,术后心肌梗死无显著降低(RR,0.809;95%置信区间,0.615 - 1.064 [P = 0.13])。根据先前研究进行了一项预先设定的亚组分析,这些研究表明丙泊酚可能会减轻RIPC的保护作用。3项研究将接受心脏手术的患者在无丙泊酚麻醉的情况下随机分为RIPC组或假手术组。这些患者大多数为男性(60.3%),平均或中位年龄在57.0至70.6岁之间。在这个434例随机分组患者的无丙泊酚亚组中,接受RIPC的217例患者中有71例(32.7%)发生AKI,而接受假手术治疗的217例患者中有103例(47.5%)发生AKI。在该队列中,RIPC使AKI显著降低(RR,0.700;95%置信区间,0.527 - 0.930 [P = 0.014])。在接受丙泊酚麻醉患者的研究中,随机分配至RIPC组的1874例患者中有445例(23.7%)发生AKI,而接受假手术的1901例患者中有474例(24.9%)发生AKI。RIPC与假手术相比,AKI的RR为0.928(95%置信区间,0.781 - 1.102;P = 0.39)。两个亚组之间无显著交互作用(P = 0.098)。
RIPC不能降低接受体外循环心脏手术患者的发病率或死亡率。在未使用丙泊酚的研究亚组中,观察到AKI有所降低,这表明丙泊酚可能与RIPC的保护作用相互作用。未来的研究应评估在无丙泊酚麻醉情况下的RIPC。