Palta Priya, Huang Elbert S, Kalyani Rita R, Golden Sherita H, Yeh Hsin-Chieh
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
Department of Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Diabetes Care. 2017 Apr;40(4):453-460. doi: 10.2337/dci16-0042. Epub 2017 Feb 21.
Hemoglobin A (HbA) level has been associated with increased mortality in middle-aged populations. The optimal intensity of glucose control in older adults with diabetes remains uncertain. We sought to estimate the risk of mortality by HbA levels among older adults with and without diabetes.
We analyzed data from adults aged ≥65 years ( = 7,333) from the Third National Health and Nutrition Examination Survey (NHANES III) (1998-1994) and Continuous NHANES (1999-2004) and their linked mortality data (through December 2011). Cox proportional hazards models were used to examine the relationship of HbA with the risk of all-cause and cause-specific (cardiovascular disease [CVD], cancer, and non-CVD/noncancer) mortality, separately for adults with diabetes and without diabetes.
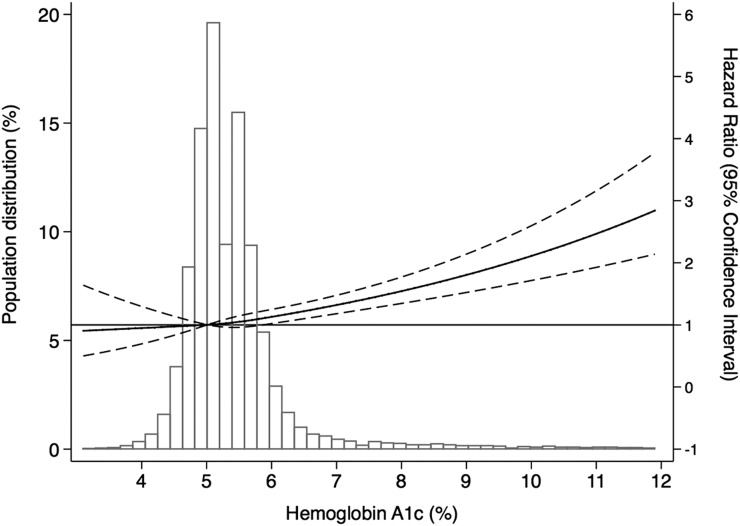
Over a median follow-up of 8.9 years, 4,729 participants died (1,262 from CVD, 850 from cancer, and 2,617 from non-CVD/noncancer causes). Compared with those with diagnosed diabetes and an HbA <6.5%, the hazard ratio (HR) for all-cause mortality was significantly greater for adults with diabetes with an HbA >8.0%. HRs were 1.6 (95% CI 1.02, 2.6) and 1.8 (95% CI 1.3, 2.6) for HbA 8.0-8.9% and ≥9.0%, respectively ( for trend <0.001). Participants with undiagnosed diabetes and HbA >6.5% had a 1.3 (95% CI 1.03, 1.8) times greater risk of all-cause mortality compared with participants without diabetes and HbA 5.0-5.6%.
An HbA >8.0% was associated with increased risk of all-cause and cause-specific mortality in older adults with diabetes. Our results support the idea that better glycemic control is important for reducing mortality; however, in light of the conflicting evidence base, there is also a need for individualized glycemic targets for older adults with diabetes depending on their demographics, duration of diabetes, and existing comorbidities.
血红蛋白A(HbA)水平与中年人群死亡率增加有关。老年糖尿病患者血糖控制的最佳强度仍不确定。我们试图评估有糖尿病和无糖尿病的老年人中HbA水平与死亡风险的关系。
我们分析了来自第三次全国健康与营养检查调查(NHANES III)(1988 - 1994年)和连续的NHANES(1999 - 2004年)中年龄≥65岁(n = 7333)的成年人的数据以及他们的关联死亡数据(截至2011年12月)。采用Cox比例风险模型分别研究糖尿病患者和非糖尿病患者中HbA与全因死亡率及特定病因(心血管疾病[CVD]、癌症和非CVD/非癌症)死亡率之间的关系。
在中位随访8.9年期间,4729名参与者死亡(1262例死于CVD,850例死于癌症,2617例死于非CVD/非癌症原因)。与已确诊糖尿病且HbA<6.5%的患者相比,HbA>8.0%的糖尿病成年人全因死亡率的风险比(HR)显著更高。HbA在8.0 - 8.9%和≥9.0%时,HR分别为1.6(95%CI 1.02,2.6)和1.8(95%CI 1.3,2.6)(趋势P<0.001)。未确诊糖尿病且HbA>6.5%的参与者与无糖尿病且HbA为5.0 - 5.6%的参与者相比,全因死亡风险高1.3(95%CI 1.03,1.8)倍。
HbA>8.0%与老年糖尿病患者全因死亡率及特定病因死亡率增加有关。我们的结果支持更好的血糖控制对降低死亡率很重要这一观点;然而,鉴于证据基础存在冲突,对于老年糖尿病患者,还需要根据其人口统计学特征、糖尿病病程和现有合并症制定个体化的血糖目标。